Purpose: The purpose of this study is to assess the COVID-19 information-seeking behavior (COVID-19 ISB) among parents in times of uncertainty and its potential association with anxiety symptoms.
Methods: Using a web-based cross-sectional survey, 306 self-selected parents participated in the study with complete responses towards the Generalized Anxiety Disorder 7-item (GAD-7) scale and COVID-19 ISB variables. Descriptive, correlation and regression analyses were applied.
Results: During the COVID-19 outbreak in Bahrain, about 18% of responding parents had moderate-severe anxiety symptoms (score ≥10 on GAD-7). The mean GAD score was 5.76±4.7. Generally, females scored a mean of (6.84±4.8), which is higher than males (4.41±4.3), (t[304] = -4.59, p ˂ .001). Participants’ utmost priority, when they sought COVID-19 information, was to know about “how to apply a proper self-quarantine”. The most relied on source for COVID-19 information was “social media accounts of health organizations”. The most restricting obstacles for seeking COVID-19 information were the “spread of rumors” and the “massive information about the disease”. The frequency of exposure to COVID-19 information was significantly associated with GAD (r[304] = 0.25, p ˂ .001). 75% of participants were satisfied with the current possibilities of acquiring COVID-19 information. This factor of satisfaction was an independent predictor for GAD, OR: 4.2 [95% CI 2.2-7.8], p ˂ 0.001.
Conclusion: The patterns and characteristics of parents’ COVID-19 ISB have the potential to influence the severity of anxiety symptoms among parents and vice versa. During epidemics, measures and strategies to reinforce a wise parent’s ISB and mitigate their anxieties must be a public health priority.
Coronavirus Disease; Health Information-Seeking Behavior HISB; General Disorder Anxiety-7; Parents, Psychometric Scale; SARS Cov-2
The pandemic outbreak of COVID-19 has imposed a critical situation of public health among the world [1]. Efforts have been directed towards ensuring appropriate levels of preparedness and response to combat the disease effectively and efficiently and to manage the ramifications associated with the outbreak [2, 3]. Families as the key building block of any society appeared to be the most important element that must be prepared adequately of how to protect itself and others from the disease and how to be capable to handle the situation in case of one of its members has become a suspected or confirmed case of COVID-19. As a result, many governments have given utmost priority to that aspect through adopting different community-based strategies like launching wide-scale COIVID-19 awareness campaigns, quarantine protocols and mandating lockdown measures including schools and workplace closures [3]. However, in the light of this worrisome situation of COVID-19 outbreak, the obvious questions arise in this context: how do parents seek COVID-19 information to be well-prepared for protecting their family and even combat the disease; and how does it impact upon anxiety levels?
Health information-seeking behavior (HISB) concept is most commonly described in the literature as an active or purposeful behavior undertaken by an individual to find information about health [4]. The concept has been frequently studied in the context of chronic diseases like diabetes and cancer [5-9]. However, limited literature is found investigating HISB among patients or healthy individuals during a disease outbreak [10]. Further, to our best of knowledge, no study has been conducted to examine HISB of parents during the COVID-19 outbreak. Hence this study dedicatedly investigates this segment of the community with regards to their information needs, sources, barriers, and satisfaction with overall existing sources. This could be of value to guide health awareness and promotion efforts in a situation facing a parallel epidemic of anxiety, panic, and depression [11]. Moreover, the WHO has disseminated clear messages emphasizing wise HISB during the COVID-19 outbreak to help to mitigate the risk of anxiety and distress feelings among people [12]. Therefore, generating empirical evidence around this aspect is largely desirable.
The Kingdom of Bahrain is one of the earliest countries that has taken clear efforts to combat and steer the COVID-19 outbreak. Going back to November, 2019, series of cases were diagnosed with novel coronavirus disease (COVID-19), first emerged and reported in Wuhan, Hubei, China. In March 2020, the pandemic spread in many countries around the world has urged the WHO to officially announce the COVID-19 outbreak a pandemic [13]. On 21 April 2020, globally, there were around 2,397,216 confirmed cases of COVID-19 and 162,956 deaths have been reported due to the outbreak of the virus [14].
By 21 April 2020, Bahrain's Ministry of Health reported that a total of 94380 samples were tested for COVID-19. The active COVID-19 cases were 1182, the stable cases: 1180, the critical cases: 2, the recoveries 784, and only death of 7 cases [15]. The government of Bahrain has taken necessary actions at multiple levels to excellently deal with the COVID-19 outbreak, and hence that it has been seen as a successful model in this aspect, as explicitly posted on Twitter by the director of WHO regional office for the Eastern and Mediterranean in March 2020: “I would like to commend Bahrain for its timely & effective preparedness & response efforts in managing COVID-19 outbreak”. The most prominent course of actions adopted by the country is the launch of Public Awareness Campaign to Combat Coronavirus disease (COVID19), which includes but not limited to large-scale COVID-19 information campaigns, inter-ministerial coordination, COVID-19 tests via mobile field units, publishing a series of guidelines of multilevel purpose, electronic registration for volunteering opportunities, and deployment of a spectrum of digital epidemiology tools for surveillance, tracking and managing the spread of the disease.
In line with the Bahrain Government efforts, it can be argued that the value of these actions can be best maximized through the way that parents being engaged in COVID-19 information seeking, which consequently could develop better awareness capacities for adherence and collaboration towards protective and precautionary measures on the one side, and better support for the family’s general health and wellbeing maintenance on the other side.
Study Subjects and Sampling
The study obtained ethical approval from the Secondary Health Care Research Sub Committee in April 2020. The researchers have also considered the American Psychological Association (APA) ethical principles of research conduct [16]. The study was conducted in the Kingdom of Bahrain which has a total population of around 1.5 million, and 264.2 thousand households according to the latest 2019 national statistics.
Nonprobability sampling (convenience sampling) was adopted for the study as it requires much less time and effort, and supports cost minimization. An unrestricted, self-selected survey which is a trending form of convenience sampling was applied [17]. This was through creating an e-survey link which was simply publicized and promoted via social media platforms; hence it was left up to each individual to choose to participate in the survey.
Potential participants, pre-accessing the questionnaire, were informed about the followings: the purpose of the survey, no known risks of participation, no monetary or non-monetary compensations on participation, data confidentiality and overall eligibility criterion of participation: Adult (>18 years old), being a parent (a mother or father of at least one child), living in the Kingdom of Bahrain, and being capable of understanding the questionnaire.
Measures and procedures
An online questionnaire in the Arabic language was used for the data collection process. The questionnaire included socio-demographic items, Generalized Anxiety Disorder – 7 (GAD-7) psychometric scale, and HISB factors. Participants’ socio-demographic data includes gender, age, and nationality, number of children, employment status, educational level, and presence of chronic disease. GAD-7 is a 7-item self-report scale (a short screening measure) used in medical and community settings to assess the severity of generalized anxiety [18]; it exhibits excellent and strong psychometric properties in terms of validity and internal consistency (Cronbach’s alpha between 0.89 and 0.92) [19-21]. Using GAD-7 scale, respondents were asked to answer how often they have been bothered by various anxiety symptoms over the last two weeks on a 4-point Liker-scale ranging from 0 (not at all sure) to 3 (nearly every day). The scale accordingly produced a total score ranged from 0 to 21. Arabic version of GAD-7 available in Patients Health Questionnaires (PHQs) website was used in this study; Arabic-translated GAD-7 measure has been verified as a reliable screening tool for anxiety through different studies in the Arabian region [22, 23].
Based on HISB concept analysis [3], five main factors were recruited in the survey instrument, related to parent’s COVID-19 information needs (9 items, 5-point rating scale), information sources (8 items, 4- point rating scale), obstacles to information seeking (7 items, 4-point rating scale), frequency of information seeking (a single item, 4-point rating scale), and degree of satisfaction for current possibilities of information sources (a single item, 4-point rating scale).
Statistical Data Analysis
As this study is based on a descriptive-correlational design, the gathered data was mainly processed through descriptive statistical analysis and inferential statistical analysis. IBM SPSS Statistics 25 was used. Cronbach’s alpha was used to estimate the reliability coefficient properties of the COVID-19 ISB survey. Procedure cross-correlation approach was utilized to establish the validity of the questions by ensuring that each HISB item is cross-correlated with the remaining questions and therefore giving assurance of the discriminant and convergent validity estimates. The descriptive statistics included means, frequency counts and percentiles which were used to describe the participants’ demographic profile, anxiety levels, COVID-19 ISB. The inferential statistics chiefly included Pearson's correlation coefficient to examine the relationship between selected COVID-19 ISB variables and anxiety symptoms severity (GAD-7). To assess the predictors of anxiety symptoms, a multivariate logistic regression model was applied; all HISB variables then entered in a multivariate logistic regression to define the independent predictors of high risk for anxiety symptoms (defined by GAD-7). Odd ratios were computed with 95% confidence intervals (95% CI).
Response Rate
As this study has adopted a convenience sampling technique, particularly via self-selection form, the response rate cannot be computed or is meaningless [24]. In general, the survey was closed when a total of 306 completed responses had been attained. This was accepted by the researchers to run the statistical tests confidently during this challenging and sensitive time of COVID-19 outbreak.
Validity and Reliability
Through analyzing the study data, the Kaiser-Meyer-Olkin (KMO) value was 0.78, indicating that the variables are adequate to correlate or to proceed with factor analysis. Bartlett’s test showed a highly significant relationship between the variables with p ˂ 0.001. Thus, the questionnaire form of the study was valid as well as the factor analysis being meaningful and acceptable [25]. Also, the internal consistency (reliability) was measured by using Cronbach’s alpha given high coefficients of 0.89 and 0.86 for the GAD-7 and COVID-19 ISB respectively.
Characteristics of Respondents
The data of the demographic profile shows that majority of the respondents were at the age bracket of 30 to 39 (42%). The majority of respondents were Bahraini citizens (79%). Employed individuals formed the largest group with 78%. Respondents having 2 to 3 children were the largest group among others with 52%. Most of respondent were holding a Bachelor degree (46%), followed by masters and doctoral degree holders 29%. In terms of medical history, most of the respondents reported not having any sort of chronic disease (67%). The details of demographic information are shown in Table 1.
Table 1. Characteristics of respondents (n = 306)
Characteristic |
no. (%) of respondents |
Sex |
|
Male |
136 (44.4) |
Female |
170 (55.6) |
Nationality |
|
Bahraini |
242 (79.1) |
Non-Bahraini |
64 (20.9) |
Age group, yr |
|
18 – 29 |
40 (13.1) |
30– 39 |
128 (41.8) |
40 – 49 |
90 (29.4) |
50 – 59 |
32 (10.5) |
≥ 60 |
16 (5.2) |
no. of children |
|
1 |
60 (19.6) |
2 - 3 |
158 (51.6) |
4 - 5 |
64 (20.9) |
≥ 6 |
24 (7.8) |
Employment status |
|
Employed |
238 (77.8) |
Unemployed |
68 (22.2) |
Education level |
|
High school or less |
26 (8.5) |
Diploma |
50 (16.3) |
Bachelor |
142 (46.4) |
Master’s and doctoral |
88 (28.8) |
Medical history |
|
Nil |
206 (67.3) |
Type 2 Diabetes Mellitus |
18 (5.9) |
Hypertension/High Blood Pressure |
24 (7.8) |
Respiratory illnesses and disease. |
8 (2.6) |
Cardiovascular disease |
12 (3.9) |
Others |
38 (12.4) |
GAD-7Related Findings
The mean GAD-7 score for the entire sample was 5.76±4.7, which indicates the prevalence of mild severity anxiety symptoms among the respondents. This was also verified through the classified percentages of GAD-7 scores showing that 18% of the participants moderate-severe anxiety symptoms. Table 2 provides an overview of overall GAD-7 results. It is worth to mention that there was a significant difference between the male group (4.41±4.3) and female group (6.84±4.8) in term of GAD scores, (t[304] = -4.59, p ˂ .001). Further, the results indicated that the larger the family size, the lesser the severity of anxiety symptoms reported by the parents (r[304] = -0.18, p ˂ .01), however the strength of this relationship was weak. Likewise, the greater age group of parents, the lesser the severity of anxiety symptoms reported by them (r[304] = -0.24, p ˂ .001). Different from our expectations, there was no difference between parents not suffering any type of chronic diseases (5.60±4.4) and their counterparts who reported having a chronic disease (6.08±5.4) in term of GAD scores, (t[162.5] = -0.77, p = .444).
Table 2. GAD-7 results in term of means, SD and frequencies (n = 306)
GAD-7 items |
M |
SD |
|
Feeling nervous, anxious, or on edge |
1.1 |
.9 |
Not being able to stop or control worrying |
0.7 |
.9 |
|
Worrying too much about different things |
0.8 |
.8 |
Trouble relaxing |
0.9 |
.9 |
Being so restless that it's hard to sit still |
0.5 |
.8 |
Becoming easily annoyed or irritable |
1.0 |
.9 |
Feeling afraid as if something awful might happen |
0.8 |
.9 |
GAD-7 mean score |
5.8 |
4.7 |
GAD-7 score |
(f, %) |
Symptom severity |
0-4 |
(142, 46.41%) |
Minimal |
5-9 |
(110, 35.95) |
Mild |
10-14 |
(34, 11.11) |
Moderate |
>15 |
(20, 6.54) |
Severe |
In this study data analysis, the participants were categorized into two groups based on: minimal to mild anxiety symptoms (score ≤ 9 on GAD) and presence of anxiety symptoms (score ≥ 10 on GAD) as shown in Table 3. The results of the logistic regression as summarized in Table 4 indicated that the independent predictors for anxiety symptoms presence were as follows:
Table 3. GAD-7 results classified according to symptoms severity (n = 306)
GAD7 category |
Freq. |
Percent |
Cum. |
Healthy (Minimal to mild) |
252 |
82.35 |
82.35 |
Moderate-severe anxiety symptoms |
54 |
17.65 |
100.00 |
Total |
306 |
100.00 |
|
Table 4. Statistical findings pertaining to COVID-19 ISB and GAD-7 (n = 306)
Domain of COVID-19 ISB |
Items |
(M±SD) |
Rank |
(r, p-value) ª |
OR [95% CI], p-valueᵇ |
|
Importance of COVID-19 information
(Rating scale: 1-5) |
About COVID19 (transmissibility, symptoms, treatment, and complications) |
(4.03±0.9) |
4 |
(0.19**, 0.001) |
0.5 [0.3-0.8], 0.008* |
Measures to protect yourself, family and others from COVID-19 infection. |
(4.33±0.8) |
3 |
(0.15**, 0.01) |
1.4 [0.6-3.0], 0.4 |
Proper diet for boosting body immunity against COVID-19. |
(3.66±1.0) |
8 |
(0.11, 0.05) |
0.8 [0.4-1.5], 0.481 |
Right ways to maintain physical activity during the COVID-19 outbreak. |
(3.23±1.3) |
9 |
(0.06, 0.30) |
.9 [0.5-1.5], 0.6 |
Effective ways to talk to your children about the COVID-19 outbreak. |
(3.80±1.0) |
7 |
(0.23**, 0.000) |
1.0 [0.6-1.8], 0.9 |
Protecting family from excessive anxiety or fear may associate with the COVID19 outbreak. |
(3.86±0.9) |
6 |
(0.16**, 0.006) |
1.9 [0.9-4.0], 0.1 |
Proper actions in case of suspecting that you or one of your family members got infected with COVID-19. |
(4.40±0.9) |
2 |
(0.09, 0.130) |
1.0 [0.4-2.6], 0.9 |
A proper way of doing self-quarantine in case it has been mandated to you or your family members. |
(4.49±0.8) |
1 |
(0.11, 0.051) |
1.1 [0.4-3.0], 0.8 |
Proper ways of managing family time at home during this outbreak of COVID-19. |
(3.95±0.9) |
5 |
(.20**, 0.000) |
1.1 [0.6-2.0], 0.8 |
|
Sources relied upon to obtain COVID-19 information
(Rating scale: 1-4) |
Broadcast media (television, radio) |
(2.61±1.1) |
6 |
(0.19**, 0.001) |
1.9 [1.1-3.2], 0.020* |
In print newspapers |
(1.64±0.9) |
8 |
(0.08, 0.157) |
1.3 [.8-2.2], 0.4 |
Social media accounts of official health organizations. |
(3.27±0.9) |
1 |
(0.15**, 0.009) |
2.3 [1.1-4.8], 0.024* |
Social media accounts of official news media |
(3.15±0.9) |
3 |
(0.15**, 0.009) |
0.7 [0.3-1.6], 0.5 |
General social media accounts |
(2.98±0.9) |
4 |
(0.18**, 0.002) |
1.0 [0.6-2.0], 0.9 |
Instant messaging applications like (WhatsApp, etc.) |
(2.65±1.1) |
5 |
(0.10, 0.092) |
1.0 [0.6-1.7], 0.9 |
People surrounding you |
(2.41±0.9) |
7 |
(0.22**, 0.000) |
1.1 [0.6-2.1], 0.8 |
Health care professionals |
(3.16±1.0) |
2 |
(0.08, 0.189) |
0.6 [0.3-1.1], 0.1 |
|
Obstacles for seeking COVID-19 information
(Rating scale: 1-5) |
The spread of false information |
(3.12±1.0) |
3 |
(0.20**, 0.000) |
2.0 [0.9-4.0], 0.1 |
Spread of rumors |
(3.23±1.0) |
1 |
(0.18**, 0.001) |
0.9 [0.4-1.9], 0.8 |
Massive information about the disease. |
(3.20±0.9) |
2 |
(0.23**, 0.000) |
0.4 [0.2-0.9], 0.029* |
shared information seems psychologically distressing |
(3.01±1.0) |
4 |
(0.44**, 0.000) |
5.6 [2.5-12.5], 0.001** |
Deficiency in trustful sources of information |
(2.71±1.0) |
5 |
(0.11*, 0.048) |
1.1 [0.6-2.1], 0.6 |
Difficulty to understand the scientific content |
(2.06±1.1) |
7 |
(0.07, 0.216) |
0.3 [0.2-0.6], 0.001** |
Time limitedness |
(2.14±1.0) |
6 |
(0.24**, 0.000) |
1.5 [0.8-2.7], 0.43 |
ª Correlation between each item of COVID-19 ISB and GAD-7 (Pearson product-moment correlation coefficient).
ᵇ Multivariate binary logistic regression analysis for predicting anxiety symptoms presence (refer to Table 3 & Graph 1) – Post-estimation Sensitivity: 44.4%, Specificity: 98.4%, Area under the Receiver Operating Characteristic (ROC) Curve: 0.85, Omnibus Tests of Model: p < 0.001.
**Significant at 0.01
*Significant at 0.05
1. The information need themed as “about COVID19 (transmissibility, symptoms, treatment, and complications)”, OR: 0.5 [95% CI 0.3-0.8], p ˂ 0.01.
2. The reliance on COVID-19 information source of “broadcast media (television, radio)”, OR: 1.9 [95% CI 1.1-3.2], p = 0.02; and source of “social media accounts of official health organizations”, OR: 2.3 [95% CI 1.1-4.8], p = 0.024.
3. The obstacles of “massive information about the COVID-19”, OR: 2.3 [95% CI 1.1-4.8], p = 0.024; “shared information seems psychologically distressing” OR: 5.6 [95% CI 2.5-12.5], p ˂ 0.001; and “difficulty to understand the scientific content”, OR: 0.3 [95% CI 0.2-0.6], p ˂ 0.001.
4. The satisfaction with COVID-19 information possibilities, OR: 4.2 [95% CI 2.2-7.8], p ˂ 0.001.
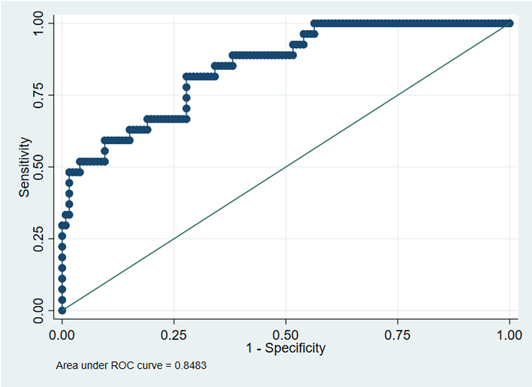
Graph 1.Receiver Operating Characteristic (Roc) Curve
Needs for COVID-19 Information
The participants indicated that the prime and most three important information subjects were: first, the “proper way of doing self-quarantine” (4.49 ±0.8); second, the “response to a COVID-19 suspected family member” (4.40±0.9); and third “COVID-19 prevention and protection measures” (4.33±0.8). The two items reported with the least importance were related to “diet for promoting immune system” (3.66±1.0) and “physical activity during COVID-19 outbreak” (3.23±1.3). Three items exhibited the highest correlation values with GAD-7, these were: “communication with children about the COVID-19” (r[304] = 0.23, p ˂ .001), “managing family time during the COVID-19 outbreak” (r[304] = 0.20, p ˂ .001), and “about COVID19 disease” (r[304] = 0.19, p ˂ .01).
Sources of COVID-19 Information
The results showed that the highest respondents’ information reliance was associated with the source of “social media accounts of official health organizations” (3.27± 0.9), followed by “health care professionals” (3.16±1.0). In contrary, the lowest respondents’ information reliance was associated with the source of “In print newspapers” (1.64±0.9), followed by “people surrounding you” (2.41±0.9) which interestingly, in comparison to its counterparts, showed the highest correlation value with the GAD-7 (r[304] = 0.22, p ˂ .001). Alongside, the second and third highest correlation was shown by the information sources of “broadcast media” (r[304] = 0.19, p ˂ .01) and “general social media accounts” (r[304] = 0.18, p ˂ .01), respectively.
Obstacles to COVID-19 Information Seeking
The results showed that the highest rated restricting obstacle was the “spread of rumors” (3.23±1.0), followed by the “massive information about the disease” (3.20±0.9). The least rating was for the obstacle of “difficulty to understand the scientific content” (2.06±1.1). The obstacle of “shared information seems psychologically distressing” displayed the highest correlation value with GAD (r[304] = 0.44, p ˂ .001).
Exposure Frequency to COVID-19 Information
In terms of how frequent the participants see or read information about the COVID19 during the day, the majority of responses were several times (61%), followed by sometimes (30%), indicating a high level of exposure to COVID-19 related information. Furthermore, the frequency of seeking COVID-19 information was significantly associated with GAD (r[304] = 0.25, p ˂ .001).
Satisfaction with COVID-19 Information
The respondents were asked about their degree of satisfaction with current possibilities of acquiring information about the COVID-19; the findings showed high satisfaction levels among them, explicitly: very satisfied (29.4%) and satisfied (46.4%). Importantly to mention in this context, it was found that higher dissatisfaction levels were associated with higher anxiety levels (r(304) = 0.20, p ˂ .01).
In general, research investigating individuals’ HISB during epidemic outbreaks has been found extensively limited in the public health literature. The intention for such investigation would become more desirable in light of evidence indicating the impact of HISB on the psychological wellbeing of individuals [26, 27]. Hence, this study, has investigated the severity of anxiety symptoms among parents and its potential association with COVID-19 ISB. This is important to fill the gap in the literature and provide valuable insights for public health actors to develop supportive and family-oriented guiding strategies for parents seeking COVID-19 information.
Our analysis of GAD-7 scores showed that the prevalence rate of moderate or severe anxiety symptoms (score ≥10 on GAD-7) was 18% which represents approximately half and two thirds of what was reported among the general Chinese population in Wuhan city 32.7% (n=167), and Shanghai city 20.4% (n=102) during the COVID-19 outbreak, respectively [28]. Also, in another study which was based on a web-based questionnaire and self-selected sampling among the Chinese population, it was found that the overall prevalence of anxiety symptoms (score ≥10 on GAD-7) was 35.1%; this was identified as a major mental health burden of the public during the COVID-19 outbreak in China [29]. However, it is not well clear whether the Chinese GAD-7 figures would be different or not from our study findings if the segment of ‘parents’ was embraced. Further, as there is lack of information on the normal levels of anxiety among the general population or parent segment in Bahrain, it is not applicable to establish a valid benchmark using our findings which are expected of being influenced by the COVID-19 outbreak. Hence, establishing public mental health dataset, including parents’ demographics, in the country would be helpful to form a strong basis for defining the extent to which the publics’ psychological state might be affected during epidemics.
In general, the high prevalence of mild anxiety symptoms among our study sample (f = 110, 35.95%) could be viewed from a positive angle as such level of anxiety severity may associate with increase public uptake of precautionary measures set by the government thereby serving as an adaptive function [28]. On the other hand, high level of anxiety can lead to adoption of irrational and maladaptive behaviors and can manifest as a pathological form of mental illness in the long term [29]. However, variances in public anxiety could be dependent on many factors like: medical resources sufficiency, health system efficiency, nature of imposed prevention and control measures, and the severity and phase of the outbreak [30]. Other studies also confirmed the cultural differences to be an important factor in shaping public responses during major health crisis [31].
Our findings revealed that the GAD-7 mean score among female group was higher than its counterpart the male group; alike with previous research revealing that women are more likely to have anxiety than men [32, 33]. Inconsistent with our expectations, the results indicated that the family size was negatively associated with anxiety symptoms among parents; this could be due to the mediating effect of social connectedness and solidarity between the family members [34]. With regard to our finding that older parents were less likely to develop anxiety symptoms; this finding is consistent with previous research suggesting that older persons had significantly lower frequencies of any current anxiety disorder and any lifetime anxiety disorder [35].
In this study, it was found that parents were in a high exposure with COVID-19 information during the day, and subsequently this may raise their anxiety symptoms. Our findings confirm previous studies inferences that increased time spent on COVID-19 information per day, particularly from social media sites, could be associated with the development of anxiety symptoms [29, 36]. However, future research investigating this aspect in line with different phases of the outbreak is important as heightened level of anxiety and avoidance of media exposure or hyperarousal behaviors may result [37].
The study respondents were in utmost need for knowing “How to apply self-quarantine”, this may reflect their worries towards the quarantine experience demanding separation from loved ones and aggravating sense of uncertainty over the disease [38]. Second, the COVID-19 information themes of significant importance for parents included “how to manage a COVID-19 suspected family member”, and “how to implement the protection measures against COVID-19”. This may infer the extent of parents’ fear from the contagiosity threat, and its perceived impact on family health status, particularly it is more likely to catch the virus from a family member besides its easy spread in households [39]. Fear or anxiety should not be seen as the only drivers for seeking COVID-19 information around these themes, perhaps awareness and personal preparedness intentions could justify the high perceptions towards these three stated themes [40].
In order to manage anxiety levels among parents, our findings imply that the needs of information relating to effective strategies for talking to the children and managing family time during the outbreak of COVID-19” should be well addressed, as parents’ perceived importance towards these subjects were found in a significant correlation with GAD. Importantly to mention within this context that increased anxiety and distress among parents can compromise their ability to recognize and respond to child emotional distress and adaptability to dramatic changes in routine, social life and study during such a crisis [41].
Two themes received the lowest scores of perceived importance, despite their significance as per the WHO recommendations, these were: “the appropriate diet for boosting body immunity” and “the right way to maintain physical activity” during the COVID-19 outbreak [42, 43]. This finding could be interpreted within the context of physical health culture in the Arabian region which is characterized by the high prevalence of inactivity among adults and children/adolescents [44], similarly with regards to the diet aspect, unhealthy dietary habits and lack of nutritional awareness are prevalent in the Arab countries [45].
The participants’ high level of dependency on reliable information channels including official social media accounts of healthcare organizations and health care providers may reflect the increased public awareness and adherence to public authorities’ recommendations for obtaining information from official sources. Additionally, the participants’ high level of satisfaction for their current possibilities of acquiring COVID-19 information which reached up to 75% can be fairly attributed to effective communication strategy adopted by Bahrain’s government to disseminate valuable and transparent situational information. As per the findings of this study, attaining high participants’ satisfaction with the accessible information sources during this epidemic crisis is desirable as it can lead to lower anxiety levels of parents and families as well as to foster favorable behavioral responses [28].
The spread of rumors, massive amount of displayed information, and distressing news were found as the top three obstacles that hinder acquiring COVID-19 information. In this study, all suggested barriers for seeking COVID-19 information were found in a significant association with parents’ anxiety levels, except the barrier of “difficulty to understand the scientific content”. The majority of these barriers have been addressed in previous research in term of their devastating impact on the psychological wellbeing of people [28, 29]. Hence, pursuing appropriate COVID-19 information publishing strategies to address public’s information needs should be a priority to reassure and rationally guide community members [46].
Our findings can reinforce public health authorities to better understand the COVID-19 ISB and its association with public psychological wellbeing, particularly in parenting and family level, hence yielding important implications for alleviating anxiety crisis provoked by epidemic outbreaks. This study brings two recommendations. First, developing an effective communication and awareness strategy that is responsive to public concerns and needs should be a high priority at the beginning of the outbreak/pandemic response efforts. This should include the monitoring of the extent and nature of content circulating on social media around the COVID-19. Second, steady and close assessment and monitoring of parents’ behaviors and mental state is inevitably important during health crises. However, these measures are dependent on the stage of the outbreak and severity of situation, besides other situational variables.
The current study has a number of limitations that dictate consideration when interpreting the findings and provide avenues for future studies. First, the psychological responses can be potentially affected by multiple factors such as other exposure to infected or suspected persons, life stressors, personality variables, previous mental health problems that were not examined in this study. Second, as the study has recruited a self-selected survey, then the generalizability of the study results to the larger population of parents needs to be carefully considered.
The main implication of this study is that it sets out important variables that could ensure wellness of parents from further mental health challenges during crisis similar to COVID-19 and even might help to prepare them for a second wave. Further research might help to develop specific parents’ tool kit for managing their children during a crisis as pandemics and the establishment of a social safety net for parent and families during national and international crises and the potential future outbreaks.
During the COVID-19 outbreak in Bahrain, the GAD-7 scores indicated that the prevalence of anxiety symptoms among parents is about 18% (score ≥10 on GAD-7). This prevalence rate appears to be quite low when the situation is compared to similar studies conducted on general populations in China as for example. Further, the study suggested a set of factors with the COVID-19 ISB deemed of vital importance to be managed through raising personal health awareness to mitigate risks of mental health burden among parents. However, mild anxiety symptoms could be seen as a motivating factor for parents to seek COVID-19 information and help protecting the health of family members.
The authors declare that they have no conflict of interest.
- World Health Organization (2020 Coronavirus Disease (COVID-19) - events as they happen. [Crossref]
- McBride O, Murphy J, Shevlin M, et al. (2020) Monitoring the psychological impact of the COVID-19 pandemic in the general population: an overview of the context, design and conduct of the COVID-19 Psychological Research Consortium (C19PRC) Study. [Crossref]
- Buheji M, Buheji A (2020) Designing Intelligent System for Stratification of COVID-19 Asymptomatic Patients. Am J Med Sci 10: 246-257. [Crossref]
- Zimmerman M, Shaw G (2020) Health information seeking behaviour: a concept analysis.
- Health Info Libr J. [Crossref]
- Longo D, Schubert S, Wright B, et al. (2010) Health Information Seeking, Receipt, and Use in Diabetes Self-Management. Ann Fam Med 8: 334-340. [Crossref]
- Kalantzi S, Kostagiolas P, Kechagias G, et al. (2015) Information seeking behavior of patients with diabetes mellitus: a cross-sectional study in an outpatient clinic of a university-affiliated hospital in Athens, Greece. BMC Res Notes 8: 48. [Crossref]
- Aldousari E (2016) Seeking Health Information in Context: An Examination Cancer Patients' Information Seeking Behavior in Kuwait. J. Soc. Sci 44: 38-58. [Crossref]
- Ghazavi Khorasgani Z, Ashrafi Rizi H, Mokarian F (2018) Health information-seeking behavior of female breast cancer patients. J Educ Health Promot 7: 138. [Crossref]
- Kimiafar K, Sarbaz M, Shahid Sales S, et al. (2016) Breast cancer patients' information needs and information-seeking behavior in a developing country. The Breast 28: 156-160. [Crossref]
- Odlum M, Yoon S (2018) Health Information Needs and Health Seeking Behavior During the 2014-2016 Ebola Outbreak: A Twitter Content Analysis. Plos Currents 10. [Crossref]
- Buheji M, Jahrami H, Dhahi A (2020) Minimizing stress exposure during pandemics similar to COVID-19. PBSIJ 10: 9-16. [Crossref]
- World Health Organization (2020) Mental health and psychosocial considerations during the COVID-19 outbreak. Geneva: WHO [Crossref]
- World Health Organization (2020) WHO announces COVID-19 outbreak a pandemic. Retrieved 14 April 2020. [Crossref]
- World Health Organization (2020) Coronavirus disease 2019 (COVID-19) Situation Report-92. Geneva: WHO. [Crossref]
- Ministry of Health (2020) Coronavirus COVID-19 - Ministry of Health. Retrieved 21 April 2020. [Crossref]
- American Psychological Association (2017) Ethical Principles of Psychologists and Code of Conduct. APA: Washington [Crossref]
- Fielding N, Lee R, Blank G (2016) The SAGE handbook of online research methods. SAGE Publications. [Crossref]
- Spitzer R, Kroenke K, Williams J, et al. (2006) A Brief Measure for Assessing Generalized Anxiety Disorder. Arch Intern Med 166: 1092. [Crossref]
- Rutter LA, Brown TA (2017) Psychometric Properties of the Generalized Anxiety Disorder Scale-7 (GAD-7) in Outpatients with Anxiety and Mood Disorders. J Psychopathol Behav Assess 39: 140-146. [Crossref]
- Johnson SU, Ulvenes PG, Øktedalen T, et al. (2019) Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample. Frontiers in psychology 10: 1713. [Crossref]
- Kertz S, Bigda Peyton J, Bjorgvinsson T (2013) Validity of the generalized anxiety disorder-7 scale in an acute psychiatric sample. Clin. Psychol. Psychother 20: 456-464. [Crossref]
- Sawaya H, Atoui M, Hamadeh A, et al. (2016) Adaptation and initial validation of the Patient Health Questionnaire - 9 (PHQ-9) and the Generalized Anxiety Disorder - 7 Questionnaire (GAD-7) in an Arabic speaking Lebanese psychiatric outpatient sample. Psychiatry Research 239: 245-252. [Crossref]
- AlHadi A, Al Ateeq D, Al Sharif E, et al. (2017) An arabic translation, reliability, and validation of Patient Health Questionnaire in a Saudi sample. Ann Gen Psychiatry 16. [Crossref]
- Leiner DJ (2017) Our Research's Breadth Lives on Convenience Samples. A Case Study of the Online Respondent Pool “SoSci Panel”. Studies in Communication | Media (SCM) 5: 367-396. [Crossref]
- Tabachnick B, Fidell L (2007) Using Multivariate Statistics Pearson/Allyn&Bacon Boston MA. [Crossref]
- McMullan R, Berle D, Arnáez S, et al. (2019) The relationships between health anxiety, online health information seeking, and cyberchondria: Systematic review and meta-analysis. J Affect Disord 245: 270-278. [Crossref]
- Musarezaie N, Samouei R, Shahrzadi L, et al. (2019) Prediction of health information-seeking behavior components based on health anxiety among users of public libraries. J Educ Health Promot 8: 227. [Crossref]
- Qian M, Wu Q, Wu P, et al. (2020) Psychological responses behavioral changes and public perceptions during the early phase of the COVID-19 outbreak in China: a population based cross-sectional survey. medRxiv. [Crossref]
- Huang Y, Zhao N (2020) Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: a web-based cross-sectional survey. medRxiv. [Crossref]
- Wind TR, Komproe IH (2012) The mechanisms that associate community social capital with post-disaster mental health: a multilevel model. Soc Sci Med 75: 1715-1720. [Crossref]
- Lin Y, Huang L, Nie S, et al. (2011) Knowledge, attitudes and practices (KAP) related to the pandemic (H1N1) 2009 among Chinese general population: a telephone survey. BMC infectious diseases 11: 128. [Crossref]
- Guo X, Meng Z, Huang G, et al. (2016) Meta-analysis of the prevalence of anxiety disorders in mainland China from 2000 to 2015. Scientific reports 6: 1-15. [Crossref]
- Gao W, Ping S, Liu X (2020) Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J. Affect. Disord 263: 292-300. [Crossref]
- Thomas P A, Liu H, Umberson D (2017) Family Relationships and Well-Being. Innovation in aging igx025. [Crossref]
- Flint AJ, Peasley Miklus C, Papademetriou E, et al. (2010) Effect of age on the frequency of anxiety disorders in major depression with psychotic features. Am J Geriatr Psychiatry 18: 404-412. [Crossref]
- Gao J, Zheng P, Jia Y, et al. (2020). Mental health problems and social media exposure during COVID-19 outbreak. Plos one 15. [Crossref]
- Collimore KC, McCabe RE, Carleton RN, et al. (2008) Media exposure and dimensions of anxiety sensitivity: Differential associations with PTSD symptom clusters. J Anxiety Disord 22: 1021-1028. [Crossref]
- Brooks SK, Webster RK, Smith LE, et al. (2020) The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. [Crossref]
- World Health Organization (2020) Household transmission investigation protocol for 2019-novel coronavirus (2019-nCoV) infection. WHO [Crossref]
- Wolf MS, Serper M, Opsasnick L, et al. (2020) Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the US Outbreak: A Cross-sectional Survey. Ann Intern Med. [Crossref]
- Dalton L, Rapa E, Stein A (2020) Protecting the psychological health of children through effective communication about COVID-19. Lancet Child Adolesc Health. [Crossref]
- World Health Organization (2020) Nutrition advice for adults during the COVID-19 outbreak. Retrieved 20 April 2020. [Crossref]
- World Health Organization. (2020). Be Active during COVID-19. Retrieved 22 April 2020. [Crossref]
- Sharara E, Akik C, Ghattas H, et al. (2018) Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC public health 18: 639. [Crossref]
- Musaiger AO, Hassan AS, Obeid O (2011) The paradox of nutrition-related diseases in the Arab countries: the need for action. Int J Environ Res Public Health 8: 3637-3671. [Crossref]
- Li L, Zhang Q, Wang X, et al. (2020) Characterizing the Propagation of Situational Information in Social Media during COVID-19 Epidemic: A Case Study on Weibo. IEEE Transactions on Computati. [Crossref]