Objective: Femoral Artery Pseudoaneurysm was caused at the puncture site of the right groin after diagnostic coronary angiography. Manual compression for 48 hours was administrated but failed then balloon tamponade was attempted for hemostasis at the aneurysmal site but hemostasis was not achieved. Next, using contralateral anterograde approach was use to cross the wire from the neck of the pseudoaneurysm and ipsilateral retrograde approach by direct puncture of the pseudoaneurysm was tried. A 0.014-inch guidewire was crossed from the neck of the pseudoaneurysm to the external iliac artery. The wire was replaced with a 0.035-inch guidewire. A star close device was inserted and was deployed at the neck of the pseudoaneurysm. Final angiography revealed completion of hemostasis.
Femoral Artery Pseudoaneurysm; Star Close
Femoral artery access is the most common approach for di- agnostic and therapeutic coronary intervention. However, puncture site complications, such as Fistula, bleeding, hema- toma and pseudoaneurysm may occur. [1]. Pseudoaneurysm is the most common femoral access complication following coronary and peripheral angiography and/or angioplasty, in- cidence ranges from 0.2% to 8% [2]. Risk factors include an- tiplatelet agents, anticoagulants, larger sheath size, puncture sitebelowcommonfemoralartery,andemergencyprocedures.
Symptoms may include groin swelling, unusual pain, bruis- ing, skin changes, neuropathy from femoral nerve compres- sion, and, rarely, limb ischemia or claudication from embo- lization or arterial compression. Rupture can be associated with severe pain and hemodynamic instability. Hence, inter- ventional cardiologists should be familiar with management. The most common nonsurgical treatment options are duplex ultrasound-guided compression, duplex ultrasound-guided Sealing pseudoaneurysms of the femoral artery with saline injection and duplex ultrasound-guided thrombin injection, which are widely used and fairly successful [3]. However, a novel approach with suture-based closure devices to treat pseudoaneurysms was recently reported.4 In this case re- port, we describe the off-label use and the long-term outcome of the Angio-Seal vascular closure device to repair a femoral pseudoaneurysm. We use new technique by using star close device with contralateral and ipsilateral approach to close the neck of the femoral pseudoaneurysm. obtained informed consent of the patient for publication of this case report.
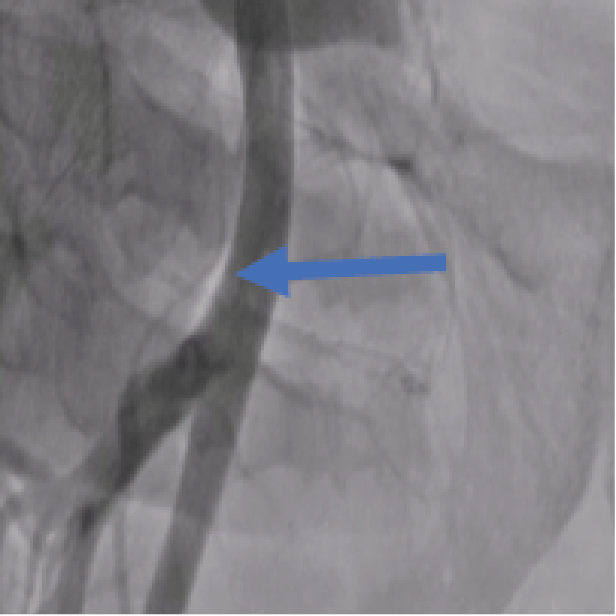
A 42-year-old male who underwent angiography with no obstructive disease found. he was discharged home on the same day but returned to the hospital for Symptoms in- clude groin swelling, unusual pain, bruising, skin changes, neuropathy from femoral nerve compression and claudica- tion from embolization or arterial compression. On examina- tion pulsatile mass in his right groin with a bruit. Angio CT suggested large pseudoaneurysm 7x8 cm in right femoral artery [figure1]. Angiography to his right common femoral artery revealed large pseudoaneurysm [2]. With a contra- lateral sheath placed in the left common femoral artery, the pseudoaneurysm was entered through the neck using 0.014 inch coronary wire. A micro introducer needle was then used to enter the pseudoaneurysm A 0.014-inch wire was then ad- vanced through the neck of the pseudoaneurysm retrograde- ly into the external iliac artery. The micro introducer sheath was then advanced into the pseudoaneurysm over the wire and retrogradely into the external iliac artery. The 0.014-inch wire was exchanged with a 0.035-inch Whole wire. The star closure device was then deployed with the anchor against the pseudoaneurysm neck with subsequent thrombosis of the pseudoaneurysm [figure 3]. Control Angiography through the contralateral sheath showed complete occlusion of the neck with no compromise to the common femoral artery.
Figure 1: CT angiography: large pseudoaneurysm in right femoral artery
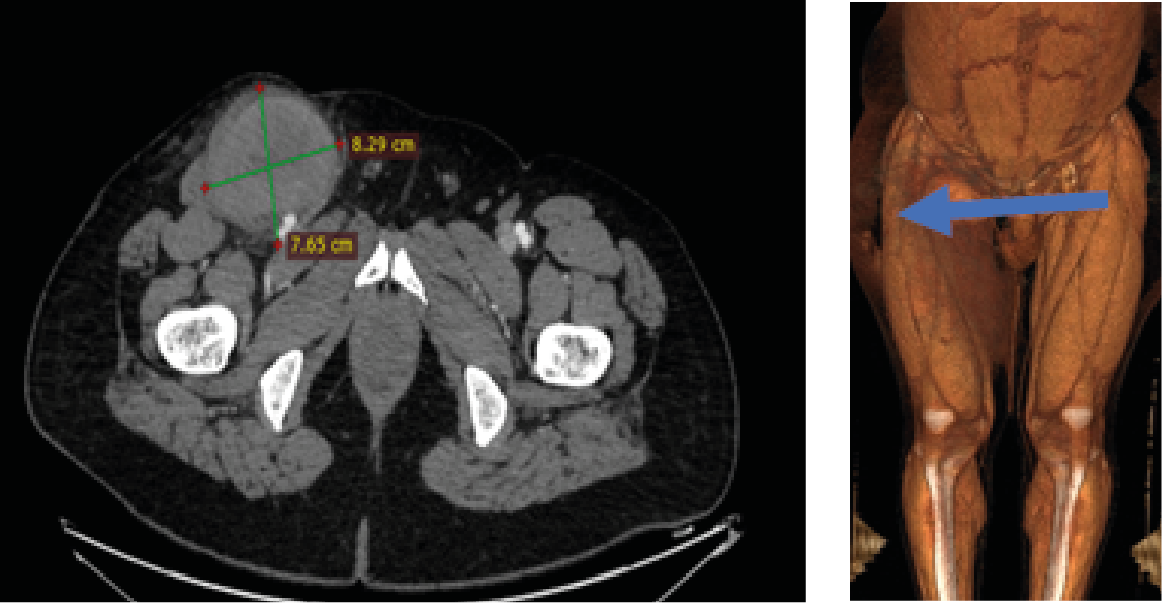
Figure 2: Selective Angiography: Pseudoaneurysm in Right Femoral Artery
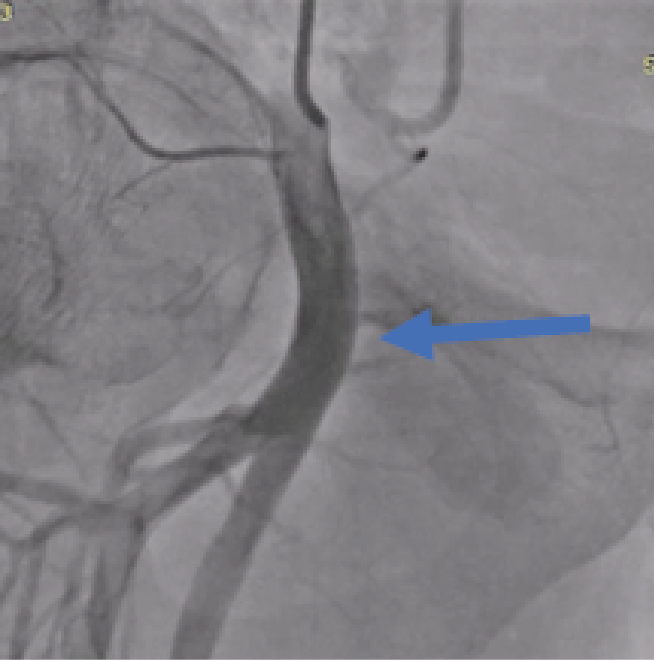
Figure 3: After Star Close Deployment, totally Occlusion in Pseudoaneurysm Neck
In this case, a novel approach to close an iatrogenic pseu- doaneurysm using the star closure device. This alternative method is likely to be useful in the setting of a large pseu- doaneurysm [> 3 mm] with a neck diameter less than 5 mm.
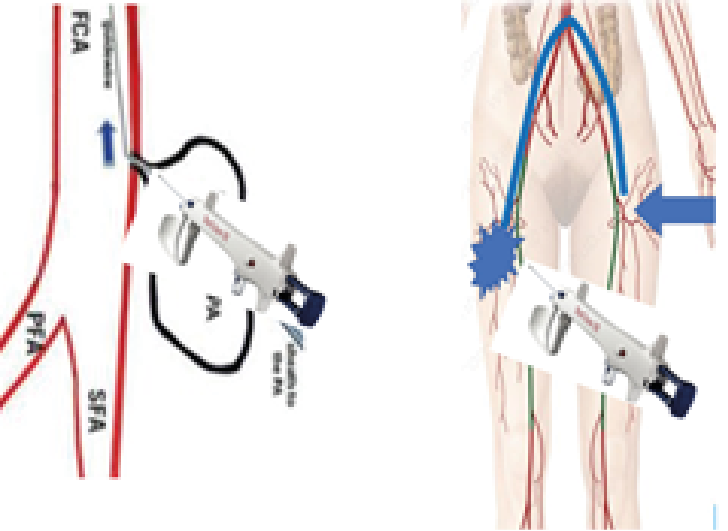
The Alshifa Hospital technique involved 4 steps to closure the neck of femoral artery pseudoaneurysm.
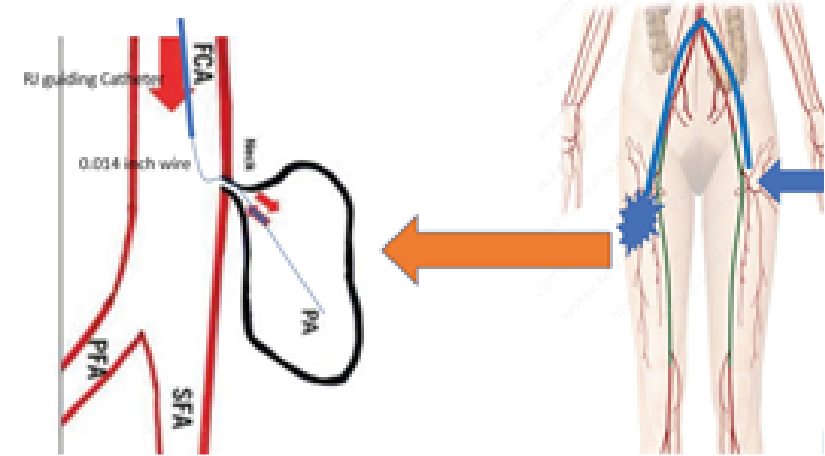
- contralteral anterograde via 3.5,6 French right Judkins guiding catheter 0.014-inch wire insertion into the femoral artery pseudoaneurysm [figure 4].
Figure 4: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
- ipsilateral retrograde via direct puncture 0.014-inch wire insertion into the external iliac artery through neck of pseu- doaneurysm [figure 5].
Figure 5: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
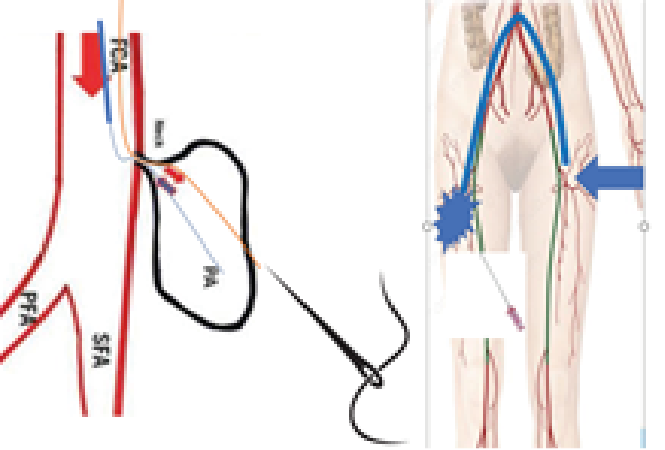
- The 0.014-inch wire was exchanged with a 0.035 inch Whole wire. The introducer sheath was then ad- vanced into the pseudoaneurysm over the wire and retrogradely into the external iliac artery [figure6].
Figure 6: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
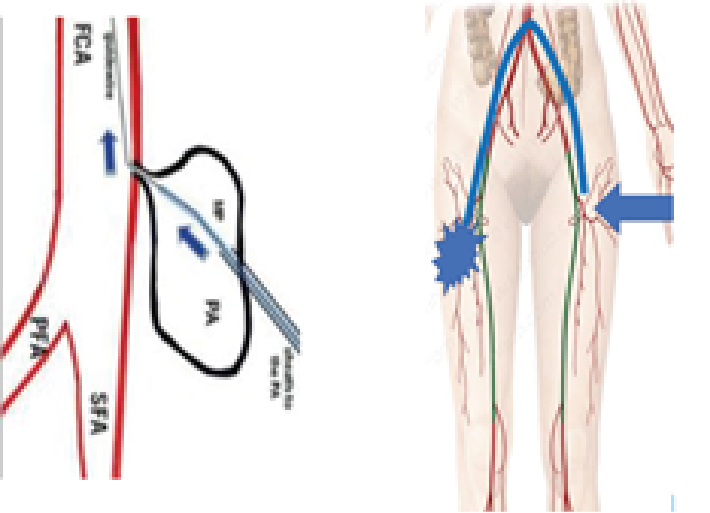
- The [star close device/or Angio cell device] was then de- ployed with the anchor against the pseudoaneurysm neck with subsequent thrombosis of the pseudoaneurysm [figure 7].
Figure 7: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
Femoral artery pseudoaneurysm is the most common com- plication of coronary and peripheral intervention. the inci- dence of pseudoaneurysm at 0.2% to 0.5% following diag- nostic procedures and up to 8% following procedures with an intervention [2]. Conservative management is an option for some patients with small femoral artery pseudoaneu- rysms.
Ultrasound-guided compression was used to treat pseudoa- neurysms, replacing surgical procedures for many pseudoa- neurysms and reporting an early success rate of 63% to 88%. [4]. Ultrasound-guided thrombin injection has replaced ultrasound-guided compression in most practices. Injection has a success rate of 93% to 97%, compared with 63% to 88% for ultrasound-guided compression. Complications of ultrasound-guided thrombin injection are rare [1.2%], with the most common being distal embolization [0.5%] [5].
Patients with large hematomas resulting in compressive symptoms such as neuropathy or ischemia and infected pseudoaneurysms are best treated with surgical repair. Surgical treatment carries a significant complication rate of 20% [6].
Our new technique has several advantages. high success rate and the most patients who are currently undergoing treat- ment with oral anticoagulants and antiplatelet agents can be successfully treated because the vascular closure device is effective independent of concomitant medications. Howev- er, we believe that this technique may be superior to throm- bin injection because potential complications that might oc- cur with thrombin injection, such as peripheral embolism of thrombin or anaphylactic reactions, are avoided, and it is less invasive than open repair.
- Bhat FA, Changal KH, Raina H, Tramboo NA, Rather HA (2017) Transradial versus transfemoral approach for coro- nary angiography and angioplastyda prospective, random- ized comparison. BMC Cardiovasc Dis. 17: 17-23. [Crossref]
- Schneider C, Malisius R, Küchler R, et al (2009) A prospective study on ultrasound-guided percutaneous thrombin injec- tion for treatment of iatrogenic post-catheterisation femoral pseudoaneurysms. Int J Cardiol.131:356-361. [Crossref]
- Webber GW, Jang J, Gustavson S, Olin JW (2007) Contempo- rary management of postcatheterization pseudoaneurysms. Circulation. 115: 2666-2674. [Crossref]
- Morgan R, Belli AM (2003) Current treatment methods for postcatheterization pseudoaneurysms. J Vasc Interv Radiol.. 14: 697-710. [Crossref]
- Taylor BS, Rhee RY, Muluk S, et al. (1999) Thrombin injection versus compression of femoral artery pseudoaneurysms. J Vasc Surg. 30:1052-1059. [Crossref]
- Webber GW, Jang J, Gustavson S, Olin JW (2007) Contempo- rary management of postcatheterization pseudoaneurysms. Circulation. 115: 2666-2674. [Crossref]