Transplantation of a tooth is often associated with the resorption of the root, frequently followed by ankylosis. In this case report, a female patient with an external root resorption following transplantation of her immature lower left premolar tooth into the socket of the upper right second premolar tooth, was investigated clinically and radiographically, and then successfully treated by the root canal medication with Calcium hydroxide (Ca(OH)2) paste. This case presentation suggested that in the case of transplantation of an immature tooth, endodontic treatment or pulp removal should be initiated as soon as the root apex is closed enough to allow preparation of the root canal, and Ca(OH)2 paste can arrest the progression of root resorption.
Root Resorption; Transplantation; Calcium Hydroxide Paste
Resorption of the root is the most common cause of tooth loss following replantation [1-3] or transplantation [4, 5]. It is initiated either outside of the tooth giving rise to external resorption or from within the pulp where it is termed internal resorption [1, 2]. Several types of external root resorption such as surface resorption, inflammatory resorption and replacement resorption (ankylosis) have already been described in many of the previous studies [6-9]. Inflammatory resorption is usually occur around the apical foramina and caused by injury to the periodontium from trauma, periodontal infection, or orthodontic treatment which initiates an inflammatory response within the periodontal ligament and leads to resorption. On the other hand, in the replacement resorption, there is a direct union between bone and root substance, and bone gradually replaces the tooth substance. This condition is diagnosed radiographically by a progressive disappearance of the periodontal ligament space and the root substance, followed by bone replacement.
Root resorption following replantation or transplantation of immature tooth could be more active and occur in a short span of years; clinical studies have reported that replanted immature teeth were lost more often and had a lower survival expectation than mature teeth in both adolescents and adults patients [1,10]. In the present case, we investigated a female patient with an external root resorption following transplantation of her immature premolar tooth, then treated by the root canal medication with Ca(OH)2 paste and observed over a period of twelve months following treatment.
A 15 years old female with an external root resorption in her upper right second premolar tooth was referred to our hospital. Her family dentist stated that the lower left first premolar tooth has been transplantated into the socket of the upper right second premolar, two and half years before, in order to reduce spacing in that side (Figure 1).
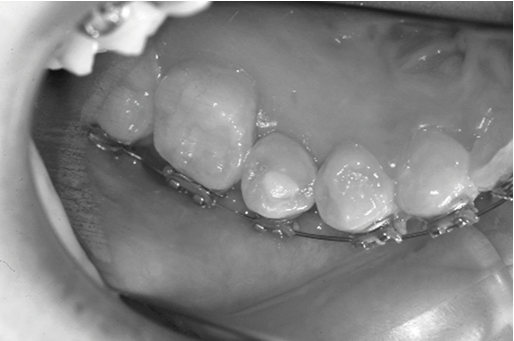
Figure 1. Oral Photograph of After Transplantation
He also stated that endodontic treatment was not performed at that time, because of the incomplete root formation of the tooth (open wide apex) and he was hoping for pulpal revascularization, followed by natural closing of the root apex. Therefore, he kept the patient under careful radiographic observation. However, one year later, as a marked external root resorption was detected by radiography, the dentist referred her to our hospital. On clinical examination, small swelling was seen on the buccal side of the effected tooth and the tooth was not tender to palpation or percussion and did not respond to electric pulp tester. Upon radiographic examination, a bowl-shaped external resorption cavity was seen with reduction of the periodontal ligament space, and there was almost completion of the root formation (Figure 2).
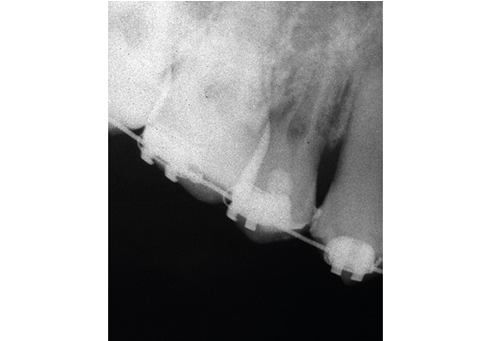
Figure 2. External Root Resorption was shown on Radiographic Examination
The affected tooth was soon subjected to endodontic treatment. Opening the pulp chamber resulted in a large amount of pus discharged and it was controlled with irrigation with sodium hypochlorite solution. The tooth was then treated as an infected root canal treatment. Rubber dam was not placed, because of the presence of the orthodontic wire in that side and therefore cotton gauge was used. The root canals were prepared using conventional technique with files and reamers (Kerr Co. Romulus, MI, USA)to a size # 50 master point wideness. Then root canal was irrigation with 3% sodium hypochlorite solution (Nippon Shikayakuhin Co. Ltd, Shimonoseki, Japan) and performed intracanal medication with Ca(OH)2 paste. The patient was recalled at once a week in the first two months, followed by once in a month for another ten months. At one year, a marked reduction in the root resorption was seen on radiographic examination, which indicated satisfactory healing. Root canal was obturated with gutta-percha point (GC Corporation, Tokyo, Japan) using the lateral condensation method (Figure 3). Thereafter the patient was kept under radiographic observation in every three months for another twelve months (Figure 4).

Figure 3. Postoperative Radiograph One Year After Root Canal Treatment With Ca(OH)2 Paste

Figure 4. Postoperative Radiograph at One Year Following Root Canal Filling
Transplantation of tooth is said as a very useful alternative method to conventional prosthetic rehabilitation or implant treatment in cases of partial edentulism [5, 12], and when appropriate conditions of the receipt site are present, it is also considered as a safe method for immature teeth [11]. Furthermore, the prognosis of transplantation has been demonstrated in several long-term clinical studies [5, 6, 11-13]. It appears from these studies that transplantation have a very good long-term prognosis, especially if performed at the proper stage of root development. A five year survival rate of 95% to 100% was found according to stage of root formation at the time of transplantation, and pulpal revascularization develops in almost all teeth after transplantation [6]. Another long term clinical results revealed 94% success rate following transplantation of immature teeth [11]. However, the risk of pulp necrosis [6] or root resorption [3-5] is very closely related to the transplantation.
In this present case, a bowl-shaped external root resorption cavity with the reduction of the periodontal ligament space and the root substance was seen radiographically following transplantation of an immature tooth. The radiographic appearance was almost similar to that of the previous studies of a replacement resorption [6], and therefore considered as a replacement type of resorption or ankylosis. Furthermore, root resorption develops within 6 months of transplantation which is also correspondent to some of the previous studies; root resorption usually diagnosed 1 to 6 months after transplantation [6]. In regards to the etiology, we considered that it is probably originated from the trauma to the periodontal ligament and the pulp tissue during the transplantation of the tooth.
Regarding the treatment, it has been reported that pulpal application of Ca(OH)2 paste has the ability to arrest external root resorption [14-15]. With the Ca(OH)2 paste, a diffusion of ions into the dentinal tubules, may cause an increase in pH, thereby influencing the resorption process at the root surface [16]. Conversely, it has been reported that calcium hydroxide therapy has no effect on replacement resorption (ankylosis) once it established [17]. In our present case, when Ca(OH)2 paste was used as an intra canal medicament during the endodontic therapy, the resorption was subsided within twelve months. Since one year has been passed after the obturation of the root canal, there is no further progression of external root resorption (Figure. 4). However, in the cases of ankylosis, ultimately there is always a risk of crown fracture of the tooth off the gingival crest as ankylosis progresses, and results in a complete replacement of the root by bone [9]. A long-term clinical evaluation is therefore necessary to determine if there is any sign for fracture in the crown. It can be suggested that following transplantation of immature tooth, endodontic treatment and pulp removal should be initiated as soon as the root apex is closed enough to allow preparation of the root canal, and Ca(OH)2 paste can arrest the progression of root resorption.
Tooth transplantation to the defect area is a very useful method. However, external resorption of the root may be occurred after transplantation.
In that case, intracanal medication with Ca(OH)2 paste is effective in reducing root resorption and promoting healing.
All authors declare no conflicts of interest in this article.
- Andreasen JO, Borum M, Jacobsen HL, et al. (1995) Replantation of 400 traumatically avulsed permanent incisors. I. Diagnosis of healing complications. Endod Dent Traumatol 11: 51-58. [Crossref]
- Andreasen JO (1993) Replantation of avulsed teeth. In: Andreasen JO, Andreasen FM (Eds.). Textbook and color Atlas of Traumatic Dental Injuries to the Teeth, 3rd edition. Copenhegen: Munsgaard. Pg no. 57-59. [Crossref]
- Majorana A, Bardellini E, Conti G, et al. (2003) Root resorption in dental trauma: 45 cases followed for 5 years. Dent Traumatol 19: 262-265. [Crossref]
- Mine K, Kanno Z, Muramoto T, et al. (2005) Occlusal forces promote periodontal healing of transplanted teeth and prevent dent alveolar ankylosis: an experimental study in rats. Angel Orthod 75: 637-644. [Crossref]
- Kim E, Jung JY, Cha IH, et al. (2005) Evaluation of the prognosis and causes of failure in 182 cases of autogenous tooth transplantation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100: 112-119. [Crossref]
- Andreasen JO, Paulsen HU, Yu Z, et al. (1990) A long-term study of 370 auto transplanted premolars Part I. Surgical procedures and standardized techniques for monitoring healing. Eur J Orthod 12: 3-13. [Crossref]
- Trope M, Yesiloy C, Koren L, et al. (1992) Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teeth. J Endod 18: 492-496. [Crossref]
- Finucane D, Kinirons MJ (2003) External inflammatory and replacement resorption of luxated, and avulsed replanted permanent incisors: a review and case presentation. Dent Traumatol 19: 170-174. [Crossref]
- Tronstad L (1985) Root resorption-Etiology, terminology and clinical manifestations. Endod Dent Traumatol 1: 221-227. [Crossref]
- Barrett EJ, Kenny DJ (1997) Survival of avulsed permanent maxillary incisors in children following delayed replantation. Endod Dent Traumatol 13: 269-275. [Crossref]
- Bauss O, Engelke W, Fenske C, et al. (2004) Autotransplantation of immature third molars into edentulous and atrophied jaw sections. Int J Oral Maxillofac Surg 33: 558-563. [Crossref]
- Mejare B, Wannfors K, Jansson L (2004) A prospective study on transplantation of third molars with complete root formation. Oral Surg Oral Med Oral Pathol Oral Radiol Endodd 97: 231-238. [Crossref]
- Bowden DE, Patel HA (1990) Autotranplantation of premolar teeth to replace missing maxillay central incisors. Br J Orthod 17: 21-28. [Crossref]
- Aqrabawi J, Jamani K (2005) Severe external root resorption arrested by conventional endodontic treatment. Dent Update 32: 224-226. [Crossref]
- Carrotte P (2004) Endodontics: Part 9. Calcium hydroxide, root resorption, endo-perio lesions. Br Dent J 25: 735-743. [Crossref]
- Trontad L, Andreasen JO, Hasselgren G, (1981) pH changes in dental tissues after root canal filling with calcium hydroxide. J Endod 7: 17-21. [Crossref]
- Foreman PC and Barnes IE (1990) A review of calcium hydroxide. Int Endod J 23: 283-297. [Crossref]