Fusion of C1-2 to treat atlantoaxial instability may be accomplished by a number of methods, but in recent years, direct screw fixation of C1-2 connected by a top-loading rods has become increasingly popular. This technique, however, may lead to a clinical problem if any excess rod is present extending superiorly above the C1 tulip head, leading to contact with the occipital bone during neck extension. A 68-year-old female with rheumatoid arthritis presented four years after C1-4 fusion for odontoid pannus formation with months of upper neck pain. CT demonstrated solid C1-2 arthrodesis but erosion of the inner cortex of the occiput by the rostral end of the rods. The rostral end of the rod was removed in revision surgery with the caudal end and C1 screws left in the bony fusion mass. The patient recovered with successful pain relief. This complication should be considered in patients with unexplained neck or occipital pain following C1-2 and below fusion surgery, and work up needs to include flexion-extension cervical spine x-rays and non-contrast CT scan. Measures to aid in complication avoidance should include careful assessment of occipital position in extension on preoperative flexion-extension x-rays and attention to the prominence of the superior hardware terminus.
atlantoaxial instability; C1-2 fusion; complication; neck pain; painful hardware
Atlantoaxial instability can result from a myriad of different pathologies including rheumatoid arthritis, Down syndrome, achondroplasia, osteogenesis imperfecta, Ehlers-Danlos syndrome, neurofibromatosis, os odontoideum, hypoplasia of the dens, ankyloses spondylitis, osteomyelitis, tumors of the craniocervical junction, and trauma to C1-C2, among other less common syndromic and non-syndromic pathologies. Fusion of C1-2 to treat atlantoaxial instability may be accomplished by a number of methods including spinous process or laminar wiring, laminar clamp techniques, and trans articular screw fixation; but in recent years, direct screw fixation of C1-2 connected by a top-loading rods has become increasingly popular as it provides excellent rigidity and does not require insertion of any hardware into the spinal canal [1-5]. This technique, however, may lead to a clinical problem if any excess rod is present extending superiorly above the C1 tulip head, as the large excursion of movement of the OC-C1 joint in flexion/extension may lead to contact of the rod tip with the occipital bone [6,7]. We illustrate a case of a patient presenting with occipital area pain caused by erosion of the occipital bone from contact with the superior tip of a rod following C1-2 fusion to treat atlantoaxial instability resulting from rheumatoid arthritis and the subsequent surgical correction.
A 68-year-old female with rheumatoid arthritis presented with months of non-radiating neck pain and worsening ambulation. Imaging demonstrated dens erosion, pannus formation, and severe cervicomedullary compression (Figure 1A, B) Dynamic x-ray imaging demonstrated significant atlantoaxial motion with 8mm atlantodental displacement. Upon movement, the atlas seemed to contact the occiput, and at rest, was only separated by 6mm. She underwent C1 laminectomy, C1 pedicle screw and C3-4 lateral mass screw placement, and bilateral C1-4 rod placement (Figure 1C, E, G). She returned four years later with complaints of upper neck pain and occipital headaches. CT demonstrated solid C1-2 arthrodesis but erosion of the occiput to the inner cortex by the rostral end of the rods, which extended beyond the C1 tulip head 1 cm on the right and 7 mm on the left (Figure 1D, F, H). At revision surgery, abundant overgrowth of bone prevented easy removal of the construct; and we chose to cut the rod with a metal-cutting burr. The inner cortex of the occipital bone was not breached and no spinal fluid leak was observed. The patient was discharged on post-operative day 2 and remained neurologically stable at 16month follow-up. The presentation of this case was approved by the institutional review board.

Figure 1a. Sagittal CT demonstrating severe erosion of the odontoid and enlarged atlantodental interval.

Figure 1b. Sagittal T2-weighted MRI demonstrating large pannus formation at the odontoid with compression of the spinal cord at the cervicomeduallary junction.
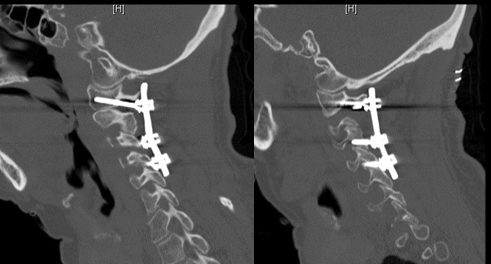
Figure 1c,1e. Left and right sagittal immediately postoperative CT images demonstrating the fusion construct from C1-C4
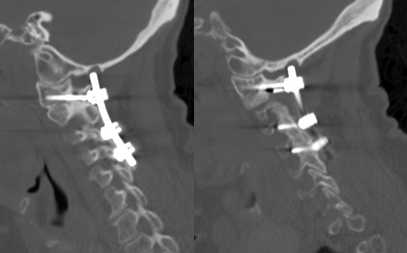
Figures 1d,1f. Sagittal 4-year postoperative images demonstrating solid fusion mass yet erosion of the occiput due to rostral rod encroachment.
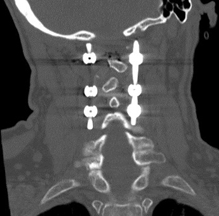
Figure 1g. coronal CT demonstrating the fusion construct.

Figure 1h. coronal CT demonstrating bilateral rod erosion of the occiput, left greater than right, with erosion to the inner cortical table on the left.
The OC-C2 area is responsible for approximately 50% of cervical spine flexion and extension, of which the OC-C1 joint makes the greatest contribution [1-8]. The wide range of sagittal movement at this level presents a challenge for a surgeon performing a C1-2 fusion: the procedure is typically performed with the patient in a neutral position, and, if movement of the occiput toward the C1 level hardware is not taken into account, a situation may be created in which the hardware may impact upon the occipital bone in extension, a phenomenon only once previously reported with rod-screw constructs [6,7]. While several postoperative complications may occur after atlantoaxial fusion, including construct failure and fracture, as well as non-union of the intended fusion segment, occipital erosion is a rare but potentially dangerous complication that many practitioners are unaware of and one that is avoidable with proper intraoperative planning in at-risk patients [9]. Given the potential for contact of the upper end of a rod with the occipital bone in extension, rods must be cut appropriately intraoperatively, and postoperatively this complication should be considered in patients with unexplained neck or occipital pain following C1-2 fusion surgery. Work up needs to include flexion-extension cervical spine x-rays and non-contrast CT scan and while cervical spine x-rays may be used as an initial screening modality, this and other studies were able to definitely demonstrate pathology only with multiplanar reconstructed computed tomography of the cervical spine [6,7]. Measures that may be helpful in avoiding this complication should include careful assessment of occipital position in extension on preoperative flexion-extension x-rays and as stated, exercising particular care in positioning fixation rods intraoperatively so that a minimum of rod projects above the C1 tulip heads.
Occipital pain with bony erosion is a potential complication of C1-2 posterior fusion with screw-rod instrumentation if excess rod contacts the occipital bone in extension, and revision surgery to trim excess prominence of the rostral end of a construct may successfully treat the symptoms. Complication avoidance measures may include careful assessment of occipital position in extension on preoperative flexion-extension x-rays and particular attention to placement of fixation rods such that a minimum of rod projects above the C1 tulip heads.
- Ma XY, Yin QS, Wu ZH, Xia H, Liu JF, et al. (2005) Anatomic considerations for the pedicle screw placement in the first cervical vertebra. Spine. 30:1519-1523. [Crossref]
- Harms J, Melcher RP (2001) Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 26:2467-2471. [Crossref]
- Melcher RP, Puttlitz CM, Kleinstueck FS, Lotz JC, Harms J, et al. (2002) Biomechanical testing of posterior atlantoaxial fixation techniques. Spine. 27:2435-2440. [Crossref]
- Huang DG, Hao DJ, He BR, Wu QN, Liu TJ, et al. (2015) Posterior atlantoaxial fixation: a review of all techniques. Spine J. 15:2271-2281. [Crossref]
- Elliott RE, Tanweer O, Boah A, Mosri A, Ma T, et al. (2013) Atlantoaxial fusion with trans articular screws: meta-analysis and review of the literature. World Neurosurg. 80:627-641. [Crossref]
- Arizumi F, Moriyama T, Tachibana T, Maruo K, Inoue S, et al. (2015) Erosion in the occipital bone caused by the fixation instrument used for posterior atlantoaxial fusion -report of 4 cases. Springerplus. 4:137. [Crossref]
- Nakao Y, Shimokawa N, Morisako H, Tsukazaki Y, Terada A, et al. (2014) Late complication of surgically treated atlantoaxial instability: occipital bone erosion induced by protruded fixed titanium rod: a case report. J Chiropr Med. 13:278-281. [Crossref]
- Gonzalez LF, Crawford NR, Chamberlain RH, Perez Garza LE, Preul MC, et al. (2003) Craniovertebral junction fixation with trans articular screws: biomechanical analysis of a novel technique. J Neurosurg. 98:202-209. [Crossref]
- Oh CH, Ji GY, Seo HS, Yoon SH, Hyun D, et al. (2014) Repeated complication following atlantoaxial fusion: a case report. Korean J Spine.11:7-11. [Crossref]