Approximately 12.4% of all diseases seen by family physicians were dermatological, and types of dermatitis represented a large proportion of these disorders. However, there are rarer skin conditions mimicking dermatitis, and there are clinical pearls to facilitate appropriate diagnosis and management decisions. For instance, angioma serpiginosum (AS) is a rare vascular disorder resembling purpura that features dilated and proliferated upper dermis capillaries. Herein we present a case of angioma serpiginosum in the upper extremity of an adolescent male which was initially misdiagnosed as atopic dermatitis and treated with topical betamethasone for two years. He was eventually referred to a dermatological specialist who suspected the possibility of angioma serpiginosum, which was confirmed by skin biopsy and histopathological analysis. Clinical pearls to distinguish AS and mimics such as atopic dermatitis, angiokeratoma, capillaritis are discussed.
Angioma Serpiginosum; Misdiagnosis; Dermatitis; Eczema; Purpura; Port-Wine Stain
It has been reported that approximately 12.4% of all diseases seen by family physicians were dermatological in nature [1]. Furthermore, a significant proportion of these skin disorders were types of dermatitis, including atopic, contact and seborrheic dermatitis, which share common treatment modalities such as topical corticosteroid application [1]. However, there are rarer dermatological conditions mimicking the appearance of dermatitis, and there are clinical pearls to facilitate the diagnosis and management decisions. Herein we present a case of angioma serpiginosum initially misdiagnosed as atopic dermatitis for two years.
Angioma serpiginosum (AS) is a rare vascular disorder resembling purpura featuring dilated and proliferated upper dermis capillaries [2]. Its prevalence is fewer than 1:1000000 [3]. Approximately 80% of cases occur before 20 years of age and 90% of cases appear in females [4]. AS is characterized by partially or non-blanchable red to violaceous punctate maculopapular lesions on an erythematous background [3]. The lesions undergo peripheral outgrowths and central clearing, resulting in serpiginous, linear or gyrate arrangements [2]. AS is a benign condition featuring slow and irregular growth which may take years [3]. These lesions are generally present asymmetrically on the lower extremities and buttocks [2]. Treatment for AS is only indicated cosmetically since AS is generally asymptomatic [3]. However, ocular and neurological complications have been previously reported [3]. Herein we describe a case of an atypical instance of angioma serpiginosum in the upper extremity of an adolescent male.
A 17-year-old male was referred from a family physician for the evaluation of an undiagnosed rash on the patient’s right arm which was unresponsive to topical betamethasone. The patient stated that the lesion originated two years ago on his right distal forearm after he took oral ibuprofen, and there was progression to his proximal forearm. He was otherwise asymptomatic. There were no remarkable events related to the onset such as trauma or exposures. He had no known allergies or drug allergies. He had no past medical history or relevant family history.
The clinical examination revealed numerous erythematous puncta in linear and serpiginous arrangement, on the extensor and flexural surfaces along the proximal and distal right forearm. At this time, the differential diagnosis included angioma serpiginosum, capillaritis (pigmented purpura), or drug eruption from ibuprofen. For diagnosis, an incisional punch biopsy was performed after obtaining informed consent from the patient. The pathology revealed non-inflammatory epidermal papillomatosis and small capillaries with mildly dilated lamina, characteristic of the dilation and proliferation of upper dermis capillaries in AS.
The patient was informed about the benign nature of the lesion and that treatment was unnecessary unless he wished to pursue laser therapy for cosmetic purposes.

Figure 1. Erythematous puncta in linear and serpiginous arrangement in the patient’s right forearm
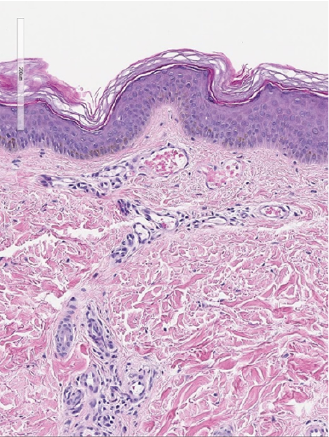
Figure 2. Dilation and proliferation of superficial papillary dermis (arrows) (H&E stain, ×20)
In this case, we presented an atypical manifestation of AS in the right arm of an adolescent male patient with progressive proximal evolution. This lesion was initially thought to be an inflammatory rash and corticosteroid creams were prescribed by the family physician, which was used intermittently by the patient. Due to the rarity of this condition, it is understandable that AS may be misdiagnosed as common inflammatory conditions such as eczema which may indicate corticosteroid therapy. Unfortunately, however, this can result in unnecessary patient exposure to the adverse effects of corticosteroids.
There are clinical pearls to facilitate the discrimination of AS from non-vascular and vascular conditions. Eczema, unlike AS, is a condition characterized by intense pruritus, xerosis, crusting, lichenification and poor circumscription [5]. Angiokeratomas may be distinguished from AS due to their rough, scaly textures [4]. Pigmented purpuric dermatoses (capillaritis) appear as orange-brown discolorations and may have a symmetrical distribution [6]. Unilateral nevoid telangiectasias are blanchable and commonly involve the C3-T1 dermatomes [4]. Port-wine stains usually appear on the face and are erythematous at birth, but become darker with age (often purple-red in adulthood) [7].
Additionally, in the case of an erythematous lesion refractory to several months of corticosteroid therapy or multiple types of topical medications, it is beneficial to pursue further workup via skin biopsy or an earlier referral to a dermatologist. This would avoid unnecessary patient exposure to adverse effects of medications and allow for earlier treatment if indicated. We hope that this discussion of an atypical patient with AS and relevant differential diagnoses will facilitate correct diagnosis in other patients.
A 17-year-old male was suffering from a progressive undiagnosed rash on his right arm for two years which was refractory to betamethasone therapy. On physical examination, there were numerous erythematous puncta in linear and serpiginous arrangement. An incisional punch biopsy and pathological analysis revealed non-inflammatory epidermal papillomatosis and capillaries with mildly dilated lamina, and the patient was diagnosed with angioma serpiginosum. This case highlights the clinical pearls used to facilitate the discrimination of AS from non-vascular and vascular conditions, and the importance of pursuing skin biopsy and referral to a dermatologist in the case of an erythematous lesion refractory to several months of corticosteroid therapy.
The authors would like to thank the patient involved in this study for their contribution to the scientific community.
The authors declare no conflicts of interest for this article.
- Verhoeven EW., Kraaimaat FW., van Weel C (2008) Skin diseases in family medicine: prevalence and health care use. Ann Fam Med 6: 349-354. [Crossref]
- Diociaiuti A., Cutrone M., Rotunno R (2019) Angioma serpiginosum: a case report and review of the literature. Ital J Pediatr 45: 53. [Crossref]
- Anjaneyan G., Kaliyadan F (2021) Angioma Serpiginosum. StatPearls. [Crossref]
- Chen JH., Wang KH., Hu CH., Chiu JS (2008) Atypical angioma serpiginosum. Yonsei Med J 49: 509-513. [Crossref]
- Siegfried EC., Hebert AA (2015) Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications. J Clin Med 4: 884-917. [Crossref]
- Morrissey K., Rosenbach M., DeHoratius D., Elenitsas R., Tetzlaff MT (2014) Granulomatous changes associated with pigmented purpuric dermatosis. Cutis 94: 197-202. [Crossref]
- Brightman LA., Geronemus RG., Reddy KK (2015) Laser treatment of port-wine stains. Clin Cosmet Investig Dermatol 8: 27-33. [Crossref]