Origin of celiac and superior mesenteric arteries from aorta through a common celiacomesenteric trunk is an infrequently revealed anatomic variation of all abdominal vascular anomalies.
Considerable anatomical variations of ventral splanchnic arteries have been very rarely seen during embryological development. Celiacomesenteric trunk is usually asymptomatic and may be discovered during vascular interventions. . It is of great significance to know the uncommon anatomic variations of celiac and superior mesenteric arteries for surgical interventions and angiographic procedures. Symptoms are rare and vary between unspecific abdominal pain and real abdominal angina.
CT angiography; Common celiacomesenteric trunk; Anatomical variation
23-year-old male came to our radiology department for renal donor CT angiography. CT angiography showed single bilateral renal arteries and veins. No area of narrowing, occlusion, aneurysm or arteriovenous malformation was identified. However, it was incidentally found that celiac and superior mesenteric arteries were arising from a single common trunk and supplying their normal territory. Figure 1 shows Common Celiacomesenteric Trunk in reformatted and 3D colored projections
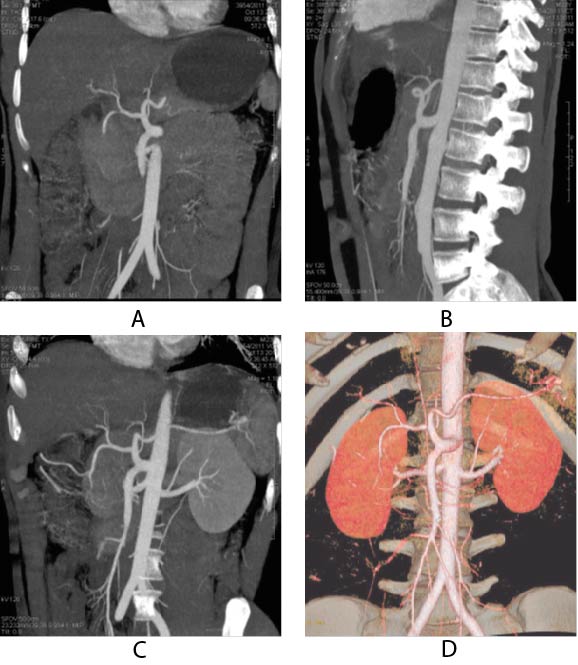
Figure 1. (A and B) Coronal and Sagittal reformatted CT angiogram shows common origin of celiac and superior mesenteric artery (|Common celiacomesenteric trunk) (C and D) Coronal reformatted CT renal angiogram with 3D colored projections shows normal renal arteries and celiacomesenteric trunk.
Amongst all the abdominal vascular anomalies, less than 1% of the cases account for the common origin of celiac and superior mesenteric artery from the aorta and it is believed that its incidence is less than 2.5%. 1-3
It is stated that the aorta is bridged to the primitive ventral anastomotic arteries by the 10th to 13th vitelline arteries. Usually the 10th and 13th vitelline roots form the celiac and superior mesenteric artery respectively, while the central ones regress along with that of ventral anastomosis. If the 10th and 12th vitelline artery regress with the persistence of large portion of ventral anastomosis a celiacomesenteric trunk is formed. The persistence of ventral anastomosis is the reason for the communication of celiac or its major branches to the superior mesenteric artery. 4-6
Crucial clinical connections are linked to this celiacomesenteric trunk origin. It is because a patient having this type of variation is now lacking the dual blood supply that is commonly present for the protection of abdominal viscera in the general population. The abdominal viscera are particularly at-risk during arthrosclerosis and complications of vascular interventional procedure. 7
Furthermore, aforementioned familiarization about the celiac trunk and superior mesenteric artery branches is necessary for attainment of successful surgeries, oncological and interventional procedures like lymphadenectomy around the hepatospleenomesenteric trunk, reimplantation of aorta and chemoembolization of liver malignancies, all of which can be at risk due to large visceral area supplied by single vessel.8
The best way to evaluate anatomy of arterial supply is through CTA. The anatomical variation detected by CTA has a diagnostic accuracy 97-98%.9 A 3D model of the arterial anatomy is made by the isotropic volume rendering and multi-planar reconstruction by the volumetric acquisition of data. Another benefit of the 3D image is the elaboration of the relationship between the arteries and the adjacent organs .9-11
These vessels supply to majority of abdominal viscera and to avoid serious vascular complications, it is essential to have knowledge about anomalous branching pattern of celiac trunk and superior mesenteric artery before any surgical, oncologic or interventional procedures including lymphadenectomy around a hepatospleenomesenteric trunk, aortic replacement with reimplantation of the trunk or chemoembolization of liver malignancies.
It is essential to acquire maximum information about variations in origin and branching patterns of celiac trunk and superior mesenteric artery before every surgical or interventional procedure in order to avoid complications and for patient’s safety. Many unintentional disasters can be avoided if their anatomic variations are known before hand to pursue proper management.
- Michels NA, Siddharth P, Kornblith PL, et al. (1968) Routes of collateral circulation of the gastrointestinal tract as ascertaines in the dissection of 500 bodies. Int Surg 49: 8-28. [Crossref]
- Michels NA (1955) Blood supply and anatomy of the upper abdominal organs with a descriptive atlas. Philadelphia: Lippincott. [Crossref]
- Fontaine R, Pietri J, Tongio J, et al. (1970) Angiographic study of the anatomic variations of the hepatic arteries based on 402 specialized examinations. Angiology 21: 110-113. [Crossref]
- Walker TG (2009) Mesenteric Vasculature and Collateral Pathways. Semin Intervent Radiol 26: 167-174. [Crossref]
- Nonent M, Larroche P, Forlodou P (2001) Celiac-Bimesenteric Trunk: Anatomic and Radiologic Description-Case Report. Radiology 220: 489-491 [Crossref]
- Song SY, Chung JW, Yin YH, et al. (2010) Celiac axis and common hepatic artery variations in 5002 patients: systematic analysis with spiral CT and DSA. Radiology 255: 278-88. [Crossref]
- Petscavage J, Maldjian P (2007) Celiomesenteric trunk: Two variants of a rare anomaly. Australasian Radiology 51: B306-B309. [Crossref]
- Losanoff JE, Millis JM, Harland RC, et al. (2007) Hepato-splenomesenteric trunk. J Am Coll Surg 204: 511. [Crossref]
- Winston CB, Lee NA, Jarnagin WR, et al. (2007) CT angiography for delineation of celiac and superior mesenteric artery variants in patients undergoing hepatobiliary and pancreatic surgery. AJR Am J Roentgenol 189: W13-19. [Crossref]
- Iezzi R, Cotroneo AR, Giancristofaro D, et al. (2008) Multidetector-row CT angiographic imaging of the celiac trunk: anatomy and normal variants. Surg Radiol Anat 30: 303-310. [Crossref]
- Crabtree R, Kirk A, Moore M, et al. (2016) Oral Health Behaviors and Perceptions among College Students. Health Care Manag 35: 350-360. [Crossref]