Trauma to the abdomen can result in various injuries, including splenic rupture or laceration. The diagnosis of a shattered spleen can be challenging as symptoms can be nonspecific, and imaging findings can be ambiguous. The Tc-99m Nano-Colloid Scintigraphy has emerged as a useful tool in the diagnosis of post-traumatic splenic injuries. In our case report, we aim to highlight the value of Tc-99m nano-colloid scintigraphy as an alternative for Tc99m sulfur colloid scan in the diagnosis of a post-traumatic shattered spleen. We presented two cases in this article who suffered from post-traumatic shattered spleen and how Tc-99m nano-colloid scintigraphy played a crucial role in their diagnosis. Both cases involved adult patients who sustained blunt abdominal trauma resulting in splenic injuries. In both cases, initial imaging was equivocal, but Tc-99m Nano-Colloid Scintigraphy revealed a shattered spleen, leading to appropriate management. In conclusion Tc-99m Nano-Colloid Scintigraphy is a cheap and readily valuable radiotracer that can assess patients and help in the management of post-traumatic shattered spleen. It can be used as a good alternative for Tc-99m sulfur colloid.
Tc99m Nano-Colloid Scintigraphy; Shattered Spleen; Splenosis; Tc99m -Sulpher Colloid Scintigraphy
Post-traumatic splenic injuries are commonly encountered in clinical practice and can range from a minor contusion to complete splenic rupture. These injuries can be life-threatening and require prompt diagnosis and treatment. However, the clinical presentation of splenic injuries can be non-specific, making their diagnosis challenging. Various imaging modalities have been used to evaluate splenic injuries, including ultrasonography, computed tomography, and magnetic resonance imaging.
Tc-99m nano-colloid scintigraphy is a nuclear medicine imaging technique that has been used in the evaluation of various liver and spleen pathologies. Tc-99m nano-colloid is a radiopharmaceutical that is taken up by reticuloendothelial cells in the liver and spleen, allowing for visualization of these organs.
In this case report, we present our local experience using Tc-99m nano-colloid scintigraphy to diagnose post-traumatic shattered spleen. We discuss two cases of patients who presented with non-specific abdominal pain following blunt abdominal trauma and were subsequently diagnosed with shattered spleen post-blunt splenic injuries using Tc-99m nano-colloid scintigraphy.
Our aim is to highlight the role of Tc-99m nano-colloid scintigraphy in the diagnosis of post-traumatic splenic injuries, particularly in cases where other imaging modalities may be inconclusive. We believe that our local experience with these cases adds to the growing body of evidence supporting the use of Tc-99m nano-colloid scintigraphy in the diagnosis of shattered spleen post-blunt splenic injuries.
A 50-year-old male presented to the adult accident and emergency department with acute onset of right flank pain. The CT scan revealed right ureteric non-obstructing calculus. In addition, an absent spleen was noted with a soft tissue nodule in the splenic fossa measuring 2 cm likely indicating a splenncule. Multiple scattered peritoneal nodules were seen in the left side of the abdomen within the mesentery, omentum, paracolic gutter, and pelvis showing a similar hyperenhancement pattern with average HU between 140-170 based on the size of the nodule. In view of the previous history of road traffic accident (RTA) and probably shattered spleen, findings were considered as splenosis, therefore the patient was sent to the nuclear medicine department for a Sulphur colloid liver-spleen scan to further characterize these lesions.
The patient was injected intravenously with 200 MBq of Tc-99m-Nanocolloid.
The study was performed using SPECT-CT Siemens Symbia T16, 15 minutes following the radiotracer injection, static mages of the chest, abdomen, and pelvis was acquired. This was followed with SPECT-CT of the same regions.
The chest and abdomen static images showed multiple foci of increased radiotracer uptake in the left upper quadrant, mid-abdomen, and pelvis which on SPECT/CT images corresponded to increased uptake along multiple scattered variable-sized well-defined soft tissue masses seen in the left side of the abdomen and splenic fossa in keeping with splenosis (Figure 1).

Figure 1: Tc99m Nano colloid scan. (A) abdomen static images showed foci of increased radiotracer uptake in the left upper quadrant and mid-abdomen and pelvis (red arrows). (B) Axial abdomen CT scan with contrast showed an absent spleen with enhancing soft tissue nodule in the splenic fossa (red arrow). (C) Axial SPECT/CT image corresponded to increased uptake along well-defined soft tissue mass seen in the splenic fossa (red arrow) in keeping with splenosis.
The partially calcified pelvic mass (which was described in the CT scan) showed increased radiotracer uptake suggestive of ectopic splenic tissue (Figure 2).
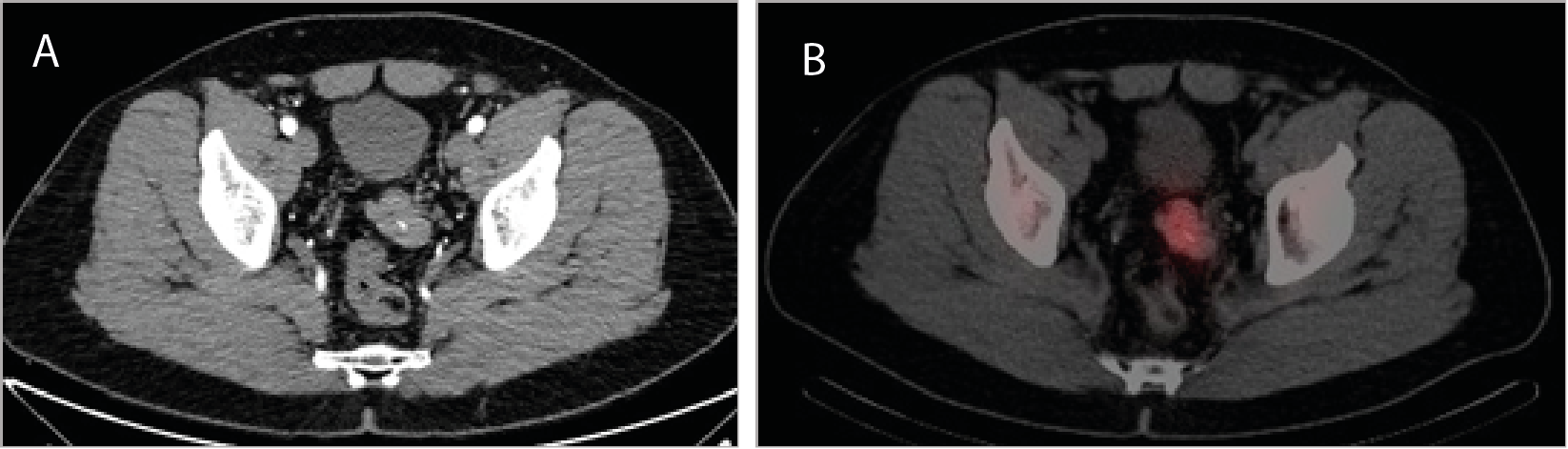
Figure 2: (A) Axial pelvis contrasted CT scan revealed a well-defined lobulated enhancing pelvic mass with foci of calcification which show increased uptake on SPECT/CT image (B) Suggestive of ectopic splenic tissue (red arrow).
In addition, there was focal abnormal radiotracer uptake seen on the left side of the chest on static images as well as SPECT images which on SPECT/CT correspond to a small sub-centimetre left upper lobe nodule (0.4 cm) (Figure 3).
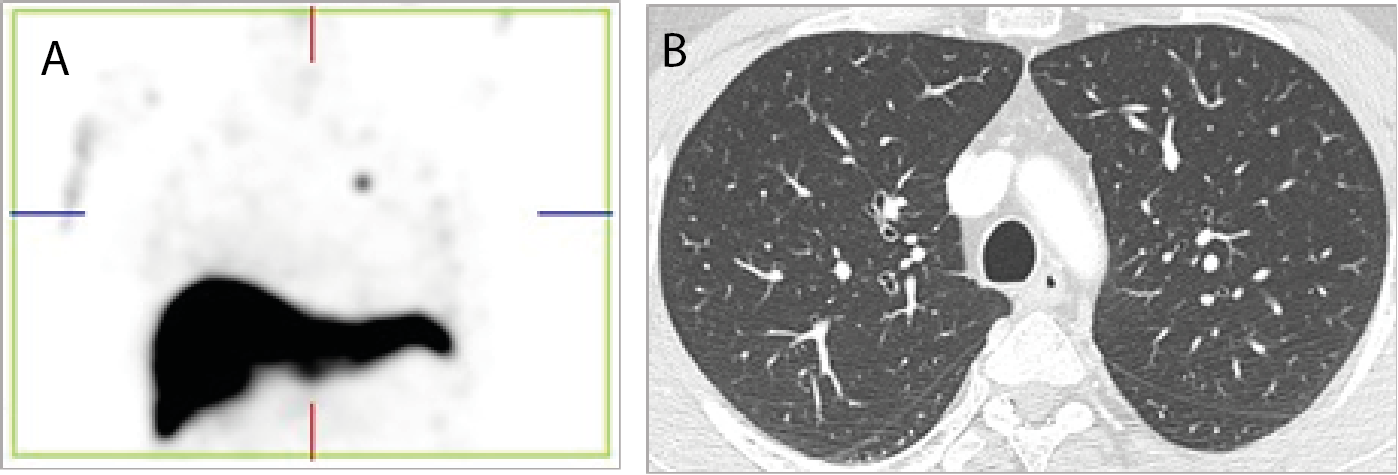
Figure 3: (A) SPECT coronal images showed focal increased uptake on the left side of the chest (red arrow) which on chest CT images (B) corresponded to a tiny pulmonary nodule on the left upper lobe (red circle) suggestive of intra-thoracic splenosis.
The second patient is a 40-year-old female who presented to the adult accident and emergency department with acute onset on abdominal pain. The CT scan revealed multiple soft tissue densities in the abdomen. This created a diagnostic challenge and a differential diagnosis of peritoneal masses was considered. However, in view of the absent spleen and previous history of RTA, she was referred to the nuclear medicine department for a Sulphur colloid liver-spleen scan to further characterize these lesions.
The patient was injected intravenously with 203 MBq of Tc-99m-Nonocolloid.
Using SPECT-CT Siemens Symbia T16, Static and SPECT-CT images of the abdomen were acquired 15 minutes following the radiotracer injection.
The study revealed normal radiotracer uptake in the liver. Multiple foci of increased radiotracer uptake were noted in the left upper quadrant and mid abdomen associated with soft tissue masses and no splenic uptake in the left upper quadrant in keeping with shattered splenic masses (Figure 4).
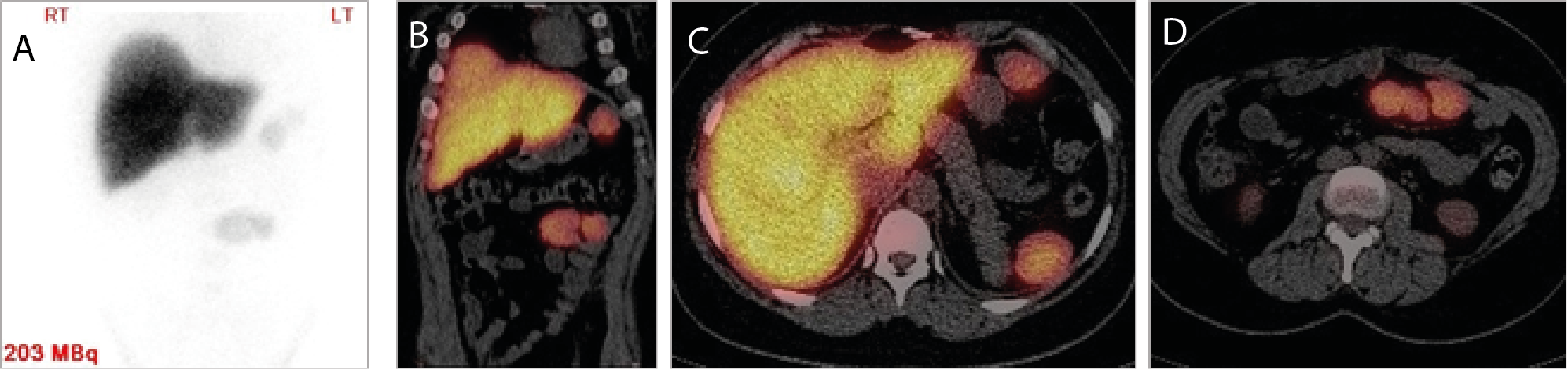
Figure 4: Tc99m Nanocolloid scan, (A) abdomen static images showed multiple foci of increased radiotracer uptake were noted in the left upper quadrant and mid abdomen (red arrows) which on SPECT/CT images (B), (C) & (D) associated with soft tissue masses in keeping with shattered splenic masses.
The spleen is the most common injured organ in blunt abdominal trauma [1]. Which can occur in contact sports, road traffic accidents, falls, and assault [2]. CT is the imaging modality of choice in the acute injury phase, acquiring the images in both arterial and venous phases to detect early vascular injury [3]. However, both of our patients had unrepairable splenic injuries for which they had to undergo splenectomy two to three decades back.
Splenosis is almost always an incidental finding in imaging [4]. As splenic tissue mimics lymphadenopathy, it might create a diagnostic dilemma and splenosis should be included in the differential diagnosis of all patients with a history of splenectomy, particularly those post blunt trauma.
In our cases, both patients presented to two different hospitals with acute abdomen and the splenosis was an incidental finding on the CT scan. Although the splenosis following splenic trauma can be seen in the abdomen and pelvis as seen in both of our cases. Thoracic splenosis seen in case first case is an uncommon clinical entity and only accounts for less than 0.25% of splenectomies [5].
Historically, Sulpher Colloid is commonly used to identify functioning splenic tissue. It consists of particles with an average size from 0.1 to 1.0 μm stabilized with gelatin. Once injected intravenously, they are phagocytized by the reticuloendothelial cells of the liver, spleen, and bone marrow in proportion to relative blood flow, functional capacity of the phagocytic cells, and particle size. The maximum concentration in the liver and spleen occurs within 10 to 20 minutes, and the rate of biological clearance from the reticuloendothelial cells is very slow [6].
In view of the international suspension of the Sulpher colloid supply, we used nano-colloid for liver-spleen imaging. In our department, we used the Nano-Colloid scan radiopharmaceutical kit. Each vial contains 0.5 mg of nano-colloidal human albumin. At least 95% of human albumin colloid particles have a diameter less than or equal to 80 nm. In both cases, the nano-colloid showed a good demonstration of splenic tissue in the abdomen, pelvis, and in a small sub-centimeter nodule in the lung.
Tc-99m Nano-colloid scintigraphy could diagnose post-traumatic shattered Spleen with good-quality images. In general, this modality can be used as a good alternative for liver spleen imaging (instead of sulfur colloid) in patients with splenosis. It is cheap and readily available and can solve a diagnostic dilemma in some patients.
- Emre Unal., Mehmet R Onur., Erhan Akpinar., Javid Ahmadov., Musturay Karcaaltincaba1., et al. (2016) Imaging findings of splenic emergencies: a pictorial review. Insights Imaging 7: 215-222. [Crossref]
- Rafailidis, V., Apostolou, D (2015) Ultrasonography of the healing process during a 3-month follow-up after a splenic injury. Ultrasonography 34: 226-231. [Crossref]
- Uyeda JW., LeBedis CA., Penn DR., Soto JA., Anderson SW (2014) Active hemorrhage and vascular injuries in splenic trauma: utility of the arterial phase in multidetector CT. Radiology 270: 99–106. [Crossref]
- Stubbs M., Aryal KR., Thomas E (2012) Paraoesophageal splenosis: An unusual differential of mediastinal soft tissue deposits. JSCR 8: 12. [Crossref]
- Niu Y., Liu W., Xian L., Tao Liu T., Huang C., et al. (2018) Thoracic splenosis presenting as pulmonary space-occupying lesion. BMC Surgery 18: 119.
- ACR–SNM–SPR (2012) Practice guideline for the performance of liver and spleen scintigraphy.