Septic arthritis in children is a serious orthopedic condition that can cause functional impairment or death through its complications. Complications are frequent and serious, in particular infective endocarditis in sepsis. We report in this paper a rare case of a 7-year-old child who had septic arthritis of the neglected ankle, complicated by severe sepsis and infectious mitral endocarditis on native valve.
Infectious Endocarditis; Septic Arthritis; Sepsis; Streptococcus
Abbreviations:
Bpm: Beats per Minute PNN: Polynuclear Neutrophil CRP: C - reactive protein ESC: European Society of Cardiology
Septic arthritis of a native joint is a frequent reason for visits to the pediatric orthopedic emergency room and is often manifested by monoarticular joint pain. The pathogens most frequently involved are Staphylococcus aureus and beta-hemolytic Streptococcus [1].
Infectious endocarditis is a sepsis condition, which constitutes the transplantation of a pathogen, on a healthy or previously damaged endocardium or on a valvular prosthesis; it is mainly responsible for valve lesions, with a significant risk of heart failure and heart failure. septic embolism. The most frequently affected valve is the mitral valve in 41% of cases, followed by the aortic valve in 38%. The clinical manifestations of endocarditis are multiple and differ according to the etiologic agent and the underlying risk factors, but none is sufficiently specific and sensitive to allow a diagnosis [2].
Child Ismail A., 7 years old, without Special pathological history presenting to the pediatric emergency room for a red, swollen, and painful right ankle (Figure 1), related to septic arthritis secondary to a neglected wound. On clinical examination: febrile at 39 °, asthenic, BP 110/70 mmHg, heart rate 130 bpm, and oxygen saturation 98%. Cardiovascular and pleuropulmonary auscultation were normal.
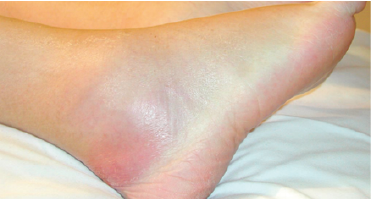
Figure 1: The Red and Swollen Ankle
On the electrocardiogram performed, sinus tachycardia was noted at 130bpm.
Biology: White blood cells at 22000 / mm3, predominantly PNN, high CRP at 270mg / l, normal renal and hepatic function, procalcitonin at 25ng / ml, with blood cultures positive for hemolytic streptococcus B.
An ankle CT scan is performed urgently and revealed osteoarthritis collected from the right ankle with multiple sequesters of the astragalus (Figure 2).
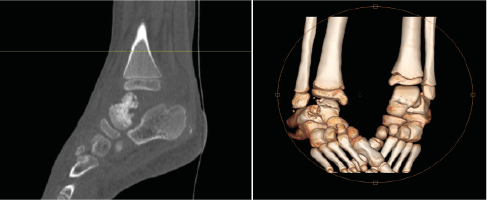
Figure 2: Scan of the Ankle with A 3D Reconstruction
The patient is transferred directly to the operating room. He underwent drainage of the ankle collection which yielded 150 ml of purulent fluid. The biological examination objectified beta-hemolytic streptococci in the drained pus.
The patient hospitalized in pediatric intensive care for the severe sespis. A transthoracic echocardiography performed systematically in our patient and diagnosed a mobile vegetation of 5 mm on the atrial side of the mitral valve (Figure 3), related to mitral endocarditis, with minimal pericardial effusion.
The diagnosis was septic arthritis of the neglected right ankle complicated by beta-haemolytic streptococcal mitral endocarditis with severe sepsis.
Child died after one week from septic shock despite treatment with antibiotics.
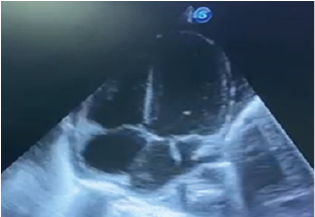
Figure 3: Apical Echocardiogram Section Showing Mitral Vegetation
The epidemiology of endocarditis has changed in the modern era. Although it remains a rare diagnosis, but the rate of infective endocarditis has increased, and it is a common concern among paediatricians [3].
However, over 90% of infectious endocarditis occurs in children with heart disease, usually congenital. Sometimes it can be a telltale sign of his heart disease [3].
Infectious endocarditis is a diagnostic and therapeutic emergency. Diagnosis is easy with typical manifestations such as prolonged fever with a heart murmur. However, the absence of a heart murmur and the presence of atypical signs (septic arthritis, glomerulonephritis, neurological complication, etc.) as the first manifestation of infectious endocarditis in an immunocompetent patient often lead to diagnostic and therapeutic delay [4].
The definitive diagnosis of infective endocarditis is based on the criteria of Durack et al at Duke University (DUKES criteria modified 2015) [5].
The entry points for infectious endocarditis are quite variable, and the most common are oral and ent as has been proven in several studies. The pulmonary route comes in second position, although it is rarely described. The other suspected entry points are urinary, gastrointestinal and skin [2]. However, septic arthritis as a gateway, such as our case, remains exceptional, and rarely described in the literature.
Septic arthritis usually presents as a tender, hot, and swollen joint or multiple joints. The most commonly affected joints are the hip and knee [1]. The germs most implicated in septic arthritis are mainly S. aureus, followed by streptococci. The knee joint is most commonly affected, followed by the elbow, shoulder, and hip [1].
Generally, and as has been described in several studies, arthralgia is the most common articular manifestation in infective endocarditis, and arthritis is rarer and may be due either to a septic localization of the sepsis or to an immunological disturbance. Septic arthritis, which is exceptional, occurs when the diagnosis is delayed or the treatment prescribed is insufficient.
Management depends on evaluating the reliability of the blood cultures, looking for underlying heart disease and identifying the portal as early as possible, especially if it is unusual. However, a neglected gateway leads to difficult or unresolvable consequences [3].
First, empiric treatment should be started, and directed to the most common germs: streptococci and staphylococci. Antibiotic therapy based on penicillin or ampicillin (or vancomycin, in case of penicillin allergy) plus gentamicin is recommended first according to the recommendations of The ESC 2015 If an organism is isolated in blood cultures, the treatment will have to be adapted.
The course may be complicated by embolization or abscess formation, heart failure, immunological complications and mycotic aneurysms.
Patients with the highest risk of complications include those with prosthetic valves, left-sided infective endocarditis, infective staphylococcal aureus or fungal endocarditis, previous episodes, duration of symptoms greater than 3 months, heart disease congenital, and poor clinical response to antibiotics [3].
In summary, clinicians should recognize septic arthritis as a possible gateway for infective endocarditis, especially in children, as illustrated in this case. And the cardiac and articular prognosis depends on the early diagnosis and the effectiveness of the treatment administered.
- Pavandeep Soor1, Nikhil Sharma1, Chandra Rao (2017) Multifocal Septic Arthritis Secondary to Infective En0docarditis: A Rare Case Report. Journal of Orthopaedic Case Reports 7: 65‑68. [Crossref]
- Mouhamadou Bamba Ndiaye, Maboury Diao, Adama Kane, et al. (2010) Infectious endocarditis in a Dakar cardiological environment: descriptive study of 39 cases Pan Afr Med J 7: 12. [Crossref]
- Andrew Hoyer, Michael Silberbach (2005) Infective Endocarditis. Pediatrics in Review 26. [Crossref]
- Madiha Mahfoudhi, Anis Hariz, Sami Turki (2014) Septic sacroiliitis revealing an infectious endocarditis. BMJ Case Rep. [Crossref]
- E B Rangel , A N Atallah (2000) Musculoskeletal manifestations of bacterial endocarditis Universidade Federal de São Paulo / Escola Paulista de Medicina, São Paulo, Brazil. Sao Paulo Med J/Rev Paul Med 118: 158-160. [Crossref]