Auto-immune thyroiditis, papillary thyroid carcinoma and primary hyperparathyroidism due to adenoma as single entities are common. Hashimoto thyroiditis is mostly related to thyroid lymphoma. Here we present the case of a 60-year-old Greek female patient presented with paresthesias of the lower extremities. Her laboratory findings were consistent with hypercalcemia, hypophosphatemia, increased urine calcium excretion and elevated parathyroid hormone levels. On suspicion of primary hyperparathyroidism with simultaneous loss of bone mass, surgical treatment was decided. She proved to suffer simultaneously from Hashimoto thyroiditis, papillary thyroid carcinoma and parathyroid adenoma. In our patient the simultaneous appearance of these three entities, Hashimoto thyroiditis, parathyroid adenoma, and papillary thyroid carcinoma, do not seem to be connected. Papillary thyroid carcinoma was an accidental finding. What is interesting about this case is that the patients’ only symptom was paresthesias of the lower extremities.
Hashimoto Thyroiditis; Hypercalcemia; Parathyroid Adenoma; Papillary Thyroid Carcinoma.
Primary hyperparathyroidism is more frequent in women over 50 years old. Adenoma is the most frequent cause (80-85% of cases), followed by hyperplasia (10–15%) and carcinoma [1]. Malignant tumors derived from the follicular epithelium are classified according to histologic features. Differentiated tumors, such as papillary thyroid cancer (PTC) or follicular thyroid cancer (FTC), are often curable, and the prognosis is good for patients identified with early-stage disease [2]. Papillary PTC is the most common type of thyroid cancer, accounting for 70–90% of well-differentiated thyroid malignancies [2].
According to the current knowledge there is no data supporting a relation between Hashimoto thyroiditis and papillary thyroid carcinoma. Hashimoto is most commonly related to thyroid lymphoma. Thyroid Lymphoma in the thyroid gland often arises in the background of Hashimoto’s thyroiditis. A rapidly expanding thyroid mass suggests the possibility of this diagnosis. Diffuse large-cell lymphoma is the most common type in the thyroid [2, 3].
A 60-year-old female Greek patient presented to her family doctor complaining about paresthesias of lower extremities. The initial laboratory tests revealed elevated serum calcium levels 11.2 mg/dL (normal values 8.2-10.4 mg/dL) and decreased serum phosphorus levels 2.2 mg/dL (normal values 2.5-4.8 mg/dL). Total proteins and serum albumin levels were normal. In the light of these results, the usual causes of hypercalcemia and hypophosphatemia where checked. The patient seemed to have normal thyroid stimulating hormone (TSH) levels 2.59 μIU/mL (normal values 0.4-4.0 μIU/mL), normal triiodothyronine (T3) levels 1.24 nmol/L (normal values 0.92-2.78 nmol/L), and normal thyroxine (T4) levels 80.64 nmol/L (normal values 58-140 nmol/L), but elevated levels of antibodies to thyroid peroxidase (anti-TPO, 1390 IU/mL (normal values <35 IU/mL)) and thyroglobulin (anti-Tg, 55 IU/mL (normal values <40 IU/mL). Parathyroid hormone (PTH) levels were elevated 123 pg/mL (normal values 5-53 pg/mL). The active vitamin D metabolite 1.25-dihydroxyvitamin D [1.25(OH) 2D3] levels, 25(ΟΗ) vitamin D levels and renal function were within normal range, and therefore secondary hyperparathyroidism was ruled out. In addition urine calcium excretion was increased and as a result the patient was considered not to suffer from familial hypocalciuric hypercalcaemia, but from primary hyperparathyroidism. Moreover there was no clinical or laboratory evidence of adrenal insufficiency, pheochromocytoma, and granulomatous diseases like sarcoidosis and tuberculosis.
Neck ultrasonography demonstrated two heterogeneous nodules in the right lobe of the thyroid gland with diameter of 21.5 mm and 21.1 mm respectively. The sestamibi scan that followed revealed diffuse increased uptake in the right thyroid lobe with high possibility of parathyroid adenoma corresponding to the mass seen on the right lobe of the thyroid gland by the ultrasound (Figure 1). The bone mass of the patient was reduced as T-score was -1.7.
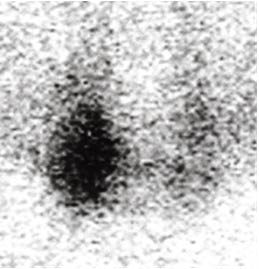
Figure 1. Sestamibi Scan Revealed Diffuse Increased Uptake in the Right Thyroid Lobe
Due to high suspicion of parathyroid adenoma combined with hypercalcemia and loss of bone mass, a parathyroidectomy and subtotal thyroidectomy of the right lobe were decided.
Histopathological examination of the excised tissue showed marked lymphocytic infiltration of the thyroid gland consistent with Hashimoto thyroiditis, papillary thyroid carcinoma of maximum diameter 0.5 cm and parathyroid adenoma.
Postoperatively the patient’s parathyroid hormone levels appeared to be normal and she became normocalcemic.
Primary hyperparathyroidism is more frequent in women and adenoma is the most frequent cause (80-85% of cases), followed by hyperplasia (10–15% of cases) and carcinoma (<1% of cases) [1].
Due to the high levels of PTH there is augmented renal resorption of calcium and phosphaturia. As a result the typical laboratory findings of a patient with primary hyperparathyroidism are hypercalcemia, hypophosphatemia, hypercalciuria, and increased levels of PTH. [1, 4] Our patient had the typical clinical manifestations and laboratory findings of primary hyperparathyroidism [4].
Strong indications of surgical removal of the parathyroid gland (parathyroidectomy) are indicated for those with symptomatic disease and are the only curative approach to the disease: severe hypercalcemia, debilitating bone disease, and PTH levels >800 pg/mL. In our patient loss of bone mass and paresthesias of the extremities due to hypercalcemia and hypophosphatemia led to the decision of surgical therapy [1].
Hashimoto thyreoiditis is an organ specific autoimmune disease and its clinical manifestations were first described by Hakaru Hashimoto in 1912. It is more often in women between 45 and 65 years old. In the contents of autoimmune polyendocrine syndromes it appears in combination with other diseases of autoimmune origin [5]. The clinical presentation of the disease varies from subclinical elevated TSH levels and the presence of autoantibodies to severe dysfunction of the thyroid gland. Genetically susceptible individuals with the HLA-DR polymorphisms HLA-DR3, -DR4, and -DR5 in Caucasians exposed to certain environmental factors as high iodine intake and decreased exposure to microorganisms in childhood is the trigger that gives genesis to marked lymphocytic infiltration of the thyroid gland. This infiltrate promotes destruction of the thyroid cells mediated by the CD8+ cytotoxic T cells. The antibodies against TPO and Tg play a secondary role by maintaining the inflammation in a thyroid cell already injured by the T cell [6]. Our patient did not have the common symptoms of hypothyroidism. The only clue to Hashimoto thyreoiditis were the elevated levels of anti-TPO and anti-Tg autoantibodies.
Papillary carcinoma is the most common differentiated carcinoma of the thyroid gland. It usually appears as a single nodule and the diagnosis is set by palpation and neck ultrasonography. Only about 5% of all thyroid nodules prove to be a malignancy [7]. Usually it appears between the ages 40 and 50 and cervical lymphadenopathy is usually present [2, 3].
According to the current knowledge there is no data supporting a relation between Hashimoto thyroiditis and papillary thyroid carcinoma. Hashimoto is most commonly related to thyroid lymphoma [2, 3].
On the other hand, simultaneous appearance of papillary thyroid carcinoma and parathyroid adenoma has been described [8, 9].
In our patient the simultaneous appearance of these three entities, Hashimoto thyroiditis, parathyroid adenoma, and papillary thyroid carcinoma, do not seem to be connected. Papillary thyroid carcinoma was an accidental finding. What is interesting about this case is that the patients’ only symptoms were paresthesias of the lower extremities.
The authors declare that they have no competing interests.
This research was supported by funding of the Department of General Surgery, St. Andrew’s General Hospital, Patras, Greece
- Saliba W, El Haddad B (2009) Secondary hyperparathyroidism: pathophysiology and treatment. J Am Board Fam Med 22: 574-581. [Crossref]
- Jameson JL, Mandel SJ, Weetman AP, Disorders of the Thyroid gland. In: Harrison’s Principles of internal Medicin19th Edition 2303-2307. [Crossref]
- Walsh S, Lowery AJ, Evoy D, et al. (2013) Thyroid lymphoma: recent advances in diagnosis and optimal management strategies. Oncologist 18: 994-1003. [Crossref]
- Khan AA, Hanley DA, Rizzoli R, et al. (2017) Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos 28:1-19. [Crossref]
- Pyzik A, Grywalska E, Matyjaszek Matuszek B, et al. (2015) Immune disorders in Hashimoto's thyroiditis: what do we know so far? J Immunol Res 2015: 979167. [Crossref]
- Jameson JL, Mandel SJ, Weetman AP. Disorders of the Thyroid gland. In: Harrison’s Principles of internal Medicin19th Edition 2290-2291. [Crossref]
- Pacini F, Castagna MG, Brilli L, et al. (2010) ESMO Guidelines Working Group. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 21: 214-219. [Crossref]
- Mahmoodzadeh H, Harirchi I, Hassan Esfehani M, et al. (2012) Papillary thyroid carcinoma associated with parathyroid adenoma. Acta Med 50: 353-354. [Crossref]
- Baumann K, Weichert J, Krokowski M, et al. (2011) Coexistent parathyroid adenoma and thyroid papillary carcinoma in pregnancy. Arch Gynecol Obstet 284: 91-94. [Crossref]