Coronavirus disease 2019 is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It has reached a global pandemic levels since March 2020. Patients with cardiovascular risk factors, acute cardiac injury and established CV disease when suffering from COVID-19, are much more vulnerable to have higher morbidity and mortality. COVID-19 has made a strong impact on health care delivery systems globally. Due to limited health resources, it has become the greatest challenge to the health systems in developing countries like Pakistan. In this study we have reviewed and discussed, how Pakistan has faced, accepted, and effectively managing this global challenge, especially in the field of Cardiology. Pakistan’s management strategy has two specific lines of action: improving clinical care and enhancement of public health services. Among general measures increasing testing capacity, tracing suspected contacts, awareness among public regarding social distancing, personal hygiene and avoiding close spaces, adoption of isolation procedures, smart lockdowns and emergency relief to the poor were the key strategic measures. For effective management of Cardiac patients, Pakistan has adopted almost all internationally recommended standard operating procedures (SOPs), especially in big cities and in tertiary care hospitals, minimizing and effectively controlling COVID-19 infection. Conclusion: Purpose of this study was to high light the fact that poor and less developed countries can very effectively improve their response capacity in crisis situations like COVID-19 by adopting simple public health measures along with few specific clinical care strategies. Moreover, research and development would address critical gaps in their health systems.
Coronavirus disease 2019 (COVID-19), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Cardiovascular Disease (CVD), Standard operating procedures (SOPs), Personal protection equipment (PPE)
Abbreviations:
Coronavirus disease 2019 (COVID-19); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); Cardiovascular Disease (CVD); Standard operating procedures (SOPs); percutaneous intervention (PCI); Personal protection equipment (PPE); Myocardial infarction (MI); Intravenous immunoglobulin (IVIG); Computed Tomography (CT).
SARS-CoV-2, like other members of the Corona viridae family, is an enveloped virus with non-segmented, single-stranded, positive-sense ribonucleic acid (RNA) genome [1]. Studies have demonstrated that SARS-CoV-2 as well as other coronaviruses can use the angiotensin-converting enzyme 2 (ACE2) protein for cell entry, providing the main entry site for the virus into human hosts [2,3].
The clinical presentation for COVID-19 is quite variable. A large study from the Chinese Center for Disease Control and Prevention demonstrated that among 72,314 patients with COVID-19 only 13.9 % subjects demonstrated severe disease and less than 5% showed critical illness [4]. Furthermore, the study showed that among confirmed cases 12.8% had hypertension, 5.3% diabetes and 4.2% had CVD [4].
Risk of Cardiovascular Disease (CVD) with COVID-19
Mechanisms that lead to cardiovascular disease (CVD) have definite overlapping with pathways that regulate immune function. Age being a strong risk factor for CVD, also affects immune functions making a person more vulnerable to COVID-19. Same is true for other CVD risk factors like diabetes and hyperlipidemia which affects immune system negatively [5-7]. It is believed and seen in few studied that higher expression of ACE2 in patients with hypertension and CVD is associated with enhanced susceptibility to SARS-CoV-2 [8].
Potential Cardiac Complications with COVID-19
Myocardial injury can occur due to myocardial ischemia or non-ischemic myocardial processes like myocarditis. They are usually represented as raised troponin levels [9-11]. Such myocardial injury has been observed in significant number of patients with severe COVID-19 respiratory infection and hypoxia. Cardiac arrhythmias can be other serious cardiac manifestation in patients with COVID-19 [12]. In one of the cohort studies, chest distress was noted in 42% and heart palpitations in 12% of the COVID positive admitted patients [13]. Heart failure was observed in 23.0% of patients with severe COVID-19 illness in one of the studies conducted in China [14].
Management Requirments
Recommended Management of Cardiac Patients with COVID-19 [15,16]
- In patients with known or suspected COVID-19, approach for management of ST-elevation myocardial infarction (MI) is same as those not having COVID. With the only difference that in the facilities where personal protection equipment (PPE) and COVID cath labs are not available, fibrinolytic therapy is preferred as compared to primary percutaneous coronary intervention (PCI), however in centers where proper PPE kits are available, primary PCI can be undertaken, keeping in mind the benefit to the patient and safety of healthcare workers.
- Delay in elective revascularization procedures should be considered in patients where the indication is just relief of symptoms.
- Studied have shown that none of the routine medications for management of coronary artery disease (CAD), including angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers have any adverse outcomes in COVID-19 infection.
- Hospital management plays pivotal role in multidisciplinary team between anesthesiologist, medical team, surgical team, infection control and intensive care to implement isolation practices.
- General management recommendations include provision of N95 mask, eye protective goggles, gown and gloves are necessary for all healthcare providers.
- Operations on confirmed positive cases should be performed in an airborne infection isolation room (AIIR).
- Drugs, anesthetic equipment, and utensils should be used only once for each patient, in order to prevent cross infection.
- Anesthesia devices to maintain airway such as laryngoscope blades, circuits, filter, respiratory balloons, and suction tubes should be discarded after single use.
- All health care providers involved in any procedure should strictly follow hospital policies regarding dispose of potential, contaminated clothing, with the aim to avoid any cross infection.
- There are certain internationally recommended general and specific guidelines for patient with or without prior CVD history in COVID-19 pandemic as shown in figure 01.
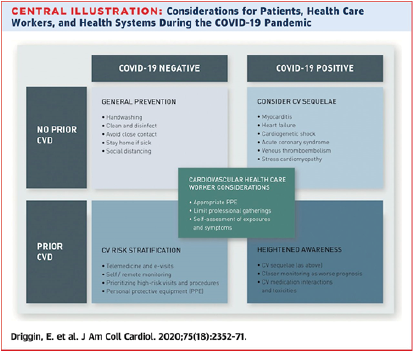
Figure 1: Recommendations and Considerations for patients and health care workers during COVID-19 [17].
Management Strategy for Cardiac Patients in Pakistan during COVID -19 Pandemic:
The management strategy of Pakistan had two distinct pathways; General measures and Specific measures: General measures included improvement in personal hygiene, Public health services and health education programs. In addition, Specific measures were taken to improve Cardiac Care Services.
Current Situation in Pakistan:
Pakistan being a developing country with limited resources had to take special steps to fight the challenge of this global pandemic. Although, health system of the country was not strong enough to cadre this serious global health issue, Government of Pakistan within its limited resources focused on increasing its testing capacity across the country, to minimize the outbreak of coronavirus.
In Pakistan, health as a subject is decentralized since 2010; for the matter like national emergency such as COVID-19, consultations are being carried out regularly among the provinces for consensus building so that a national coherent response to COVID-19 could be achieved. Due to strict and timely actions of Government in relation with the quarantine, tracing suspected contacts and adoption of isolation procedures, Pakistan managed to come out of first phase of COVID-19 successfully keeping the total death toll extremely low due to its effective management strategy [17].
At the end of 2020, government of Pakistan has officially confirmed that the second wave of COVID-19 has started in the country as shown in figure 02. As per official statements, Pakistan is now witnessing more than 1000 COVID-19 cases daily. As many as 2475 new COVID-19 cases were reported in Pakistan on 30th of December 2020, taking the country's total tally to 479,715 [18]. The number of active COVID-19 cases in Pakistan had dropped to 6,000 in September. So as per statistics the problem is once again increasing in the country. Government of Pakistan, in this second phase, is planning to utilize the same strategy i.e., increasing testing capacities, tracing suspected patients, smart lockdowns and emergency relief to the poor, which was proved to be highly effective in first phase of pandemic.
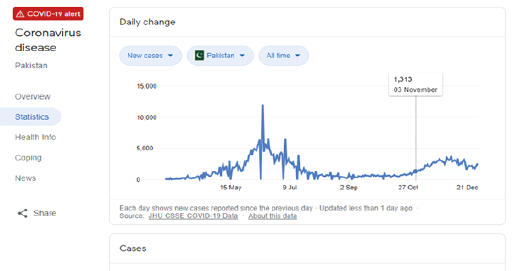
Figure 2: Current statistics of COVID-19 in Pakistan showing second phase [18].
Methodology to Improve Response Capacity:
Following General Measures opted by the Government to minimize the spread of Infection:
- In Pakistan, percentage of GDP in health sector had been less than 1% for decades. In 2019, 12,671 million rupees were allocated for development in the health sector [19].
- One serious issue is delay in presentation due to lack of education and miss information. Delayed presentation is a serious concern especially in cardiovascular (CV) emergencies where patients are afraid to seek medical attention during the pandemic. Government of Pakistan has established its official website and has involved electronic and print media for health education regarding COVID-19; so that all miss information could be dealt with adequately.
- Pakistan has doubled it ventilation support capacity through-out the country, within last one year.
- Government of Pakistan has launched Ehsas Program to provide direct financial support to the poor [20], in addition they have also launched Health insurance facility by the name of Sehat Sahulat Program so that poor especially those suffering from COVID can get best available healthcare facilities on government expenses.
- Pakistan is establishing and improving its Tele-health capabilities, so that relatively less sick patient can get medical advice without leaving their homes, another effort to minimize chance of cross infection.
- In addition, Government of Pakistan has already started COVID-19 vaccination of their health care providers, in all the major cities, of all four provinces.
Specific Measures to Improve Cardiac Health Care:
This information has been collected from two hospitals in Islamabad, Pakistan.
Federal Government Polyclinic Hospital, Islamabad, a public sector, tertiary care hospital and Kulsum International Hospital, Islamabad; dedicated Cardiac, tertiary care, private hospital in Islamabad.
As per international recommendations in patients with known or suspected COVID-19, approach for management of ST-elevation myocardial infarction (MI) was same as those not having COVID.
- In Pakistan there are many centers where cardiac patients are being treated but they do not have cath labs, especially in present scenario they do not have dedicated COVID cath labs. So, they prefer using fibrinolytic therapy rather than primary percutaneous coronary intervention (PCI) and this is the recommendation scheme of action in COVID-19.
- In bigger cities, there are centers both in public and private sector, where COVID cath labs and proper PPE kits are available. In such set-up intervention is being done regularly and successfully, avoiding spread of COVID infection, and keeping in mind the safety of healthcare workers.
- It was observed that COVID testing was a must pre-requirement before any intervention, as per international recommendations.
- In every tertiary care hospital, where major interventions are being done, there was a team of healthcare providers which includes at least a pulmonologist, an infectious diseases expert and a critical care specialist. It is the responsibility of entire team to take care of critically ill COVID-19 patients and when these critical COVID patients are cardiac patients, interventional cardiologist is essential part of the team.
- Dedicated tertiary care hospitals have COVID cath labs and for confirmed positive cases airborne infection isolation room. They follow recommended SOPs for use of anesthesia equipment, utencils and drugs etc, with the aim to minimize the spread of COVID infection.
- Though not in every tertiary care hospital but still in many hospitals especially in big cities advance diagnostic facilities like chest CT are available. Sometimes it is not possible to completely rule in or rule out the possibility of COVID-19 on chest CT findings [21], still it is of great help in management of hospitalized patients especially when they have other serious diagnoses like cardiovascular disease.
Ongoing Research Activities for Covid-19:
As part of future management strategy Pakistan realizes that there is urgent need of high-quality research in the field of COVID-19. A team of scientists from the Dow University of Health Sciences (DUHS) prepared intravenous immunoglobulin (IVIG) with plasma obtained from recovered coronavirus patients [22]. It was done in April 2020 and was successfully used in many COVID patients.
Many other researchers are actively involved in research all over Pakistan. According to a statement from the national institute of health (NIH), it has obtained approval from the drug regulatory authority of Pakistan for phase-III Clinical Trial of Recombinant Novel Coronavirus Vaccine Adenovirus Type 5 vector (Ad5-nCoV) developed by CanSinoBio and Beijing Institute of Biotechnology China [23].
Purpose of this study was to high light the fact that poor and less developed countries can very effectively improve their response capacity in crisis situations like COVID-19 by adopting simple public health measures along with few specific clinical care strategies. Moreover, research and development would address critical gaps in their health systems.
Patients were not directly involved therefore informed written consent was not obtained.
This study was not funded by any organization.
- Cui J, Li F, Shi ZL (2019) Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol 17: 181-192. [Crossref]
- Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, et al. (2020) Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 181: 281-292. [Crossref]
- Li W, Moore MJ, Vasilieva N, Sui J, Wong SK, et al. (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426: 450-454. [Crossref]
- Zhonghua Liu Xing Bing Xue Za Zhi (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Epidemiology Working Group for Ncip Epidemic Response CCfDC, Prevention. 41: 145-151.
- Spezzani V, Piunno A, Iselin H-U (2020) Benign COVID-19 in an immunocompromised cancer patient - the case of a married couple. Swiss Med Wkly [Crossref]
- Wang X, Fang X, Cai Z, Wu X, Gao X, et al. (2020) Comorbid chronic diseases and acute organ injuries are strongly correlated with disease severity and mortality among COVID-19 patients: a systemic review and meta-analysis. Research (Wash D C) 2020: 2402961.
- Guzman-Flores JM, Lopez-Briones S (2012) Cells of innate and adaptive immunity in type 2 diabetes and obesity. Gac Med Mex 148: 381-389.
- Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, et al. (2020) Cardiac Involvement in a Patient with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol 5: 819-824. [Crossref]
- Guo T, Fan Y, Chen M, Wu X, Zhang L, et al. (2020) Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol 5: 811-818. [Crossref]
- Shi S, Qin M, Shen B, Cai Y, Liu T, et al. (2016) Association of Cardiac Injury with Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol 5: 801-810. [Crossref]
- Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O (2020) Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol 5: 831-840. [Crossref]
- National Health Society. NHS Clinical guide for the management of cardiology patients during the coronavirus pandemic. https://www.england.nhs.uk/coronavirus/publication/specialty-guides/ (April 1, 2020; date last accessed).
- Qu G, Chen J, Huang G, Zhang M, Yu H, et al. (2021) A quantitative exploration of symptoms in COVID-19 patients: an observational cohort study. Int J Med Sci 18: 1082-1095.
- Zhou F, Yu T, Du R (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 6736: 1-9. [Crossref]
- Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 323: 1061-1069.
- Musher DM, Abers MS, Corrales-Medina VF (2019) Acute infection and myocardial infarction. N Engl J Med 380: 171-176. [Crossref]
- Driggin E, Madhavan MV, Bikdeli B, Chuich T, Laracy J, et al. (2020) Cardiovascular Considerations for Patients, Health Care Workers, and Health Systems During the COVID-19 Pandemic. J Am Coll Cardiol 75: 2352-2371. [Crossref]
- Pakistan COVID-19 Health Advisory Platform by Ministry of National Health Services. covid.gov.pk/stats/Pakistan.
- ES Health and Nutrition 2019. Available from: http://www.finance.gov.pk/survey/chapters_1 9/11-Health and Nutrition.pdf .
- Develop the Ehsaas strategy-the first coordinated whole-of-government approach to addressing poverty and inequality. Ehsaas Governance and Integrity Policy. http://pmo.gov.pk/documents/Ehsaas-Governance-Policy.pdf.
- Yang W, Cao Q, Qin L, Wang X, Cheng Z, et al. (2020) Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. J Infect 80: 388-393. [Crossref]
- Shaukat A, Shobha L, Fatima A, Sheikh MM (2020) Hyper-immune anti-COVID-19 IVIG (C-IVIG) Therapy for Passive Immunization of Severe and Critically Ill COVID-19 Patients: A structured summary of a study protocol for a randomized controlled trial. Trials 21: 905.
- Pakistan to conduct phase-III clinical trial of Covid-19 vaccine. Health world.com, from Economic times. August 19, 2020, https://health.economictimes.indiatimes.com/news/industry/pakistan-to-conduct-phase-iii-clinical-trial-of-covid-19-vaccine/77631143.