Myocardial contusion is a frequent but often underestimated complication of blunt chest trauma. It involves cellular damage following non-penetrating thoracic trauma. It is commonly observed after road traffic accidents but can occur with any type of blunt thoracic trauma. We present a case of myocardial contusion following a road traffic accident in a 22-year-old male patient with no medical history, who was admitted to the emergency resuscitation room for severe trauma due to a road traffic accident. The lesion assessment revealed multiple pulmonary contusions in the thoracic area, with a moderate right-sided pneumothorax and a small left-sided pneumothorax, a right posterior basal hemothorax, and a large pneumomediastinum. The initial Electrocardiogram (ECG) showed no abnormalities apart from sinus tachycardia. Transthoracic echocardiography (TTE) revealed left ventricular hypokinesia with a normal right ventricle. Troponin levels were elevated at 7 ng/mL. Initial management included two peripheral venous lines, fluid resuscitation, oxygen therapy, and right pneumothorax decompression. Clinical and biological outcomes were favorable.
Chest Trauma; Myocardial Contusion; Troponin; Electrocardiogram
Myocardial contusion is a potential complication of cardiac trauma [1]. Its incidence varies greatly due to its clinical polymorphism and the frequent presence of associated lesions that may mask the initial diagnosis [3-5]. Its morbidity and mortality are not negligible. This paper reports a case of post-traumatic myocardial contusion with clinical, electrical, biological, and echocardiographic repercussions [6, 8, 9].
We report the case of a 22-year-old male with no medical history who was admitted to the emergency resuscitation room following severe trauma due to a road traffic accident. On admission, respiratory rate was 26 breaths/min, with significant subcutaneous emphysema involving the cervical, thoracic, and abdominal regions, associated with thoracic deformity and evident signs of right-sided pneumothorax. Blood pressure was 60/42 mm Hg, heart rate 132 bpm, and heart sounds were normal. Temperature was 37.4°C and capillary blood glucose 1.06g/dL.
Initial management included insertion of two peripheral venous lines, fluid resuscitation, oxygen therapy, and decompression of the right pneumothorax. The thoracic injury assessment revealed multiple pulmonary contusions, a moderate right pneumothorax, a small left pneumothorax, a right posterior basal hemothorax, and a large pneumomediastinum on chest CT scan (Figures 1, 2, and 3). In addition, extensive subcutaneous emphysema was noted in the thoracic and dorsal softs tissues.
Initial ECG showed no abnormalities apart from sinus tachycardia (Figure 4). Transthoracic echocardiography revealed left ventricular hypokinesia; the right ventricle was normal. Troponin levels were elevated at 7 ng/mL. Internal milieu laboratory parameters were unremarkable. Due to persistent hemodynamic instability, dobutamine was initiated along with cautious fluid resuscitation. Clinical and biological progress was favorable, including weaning of catecholamines and normalization of troponin levels after 8 days.
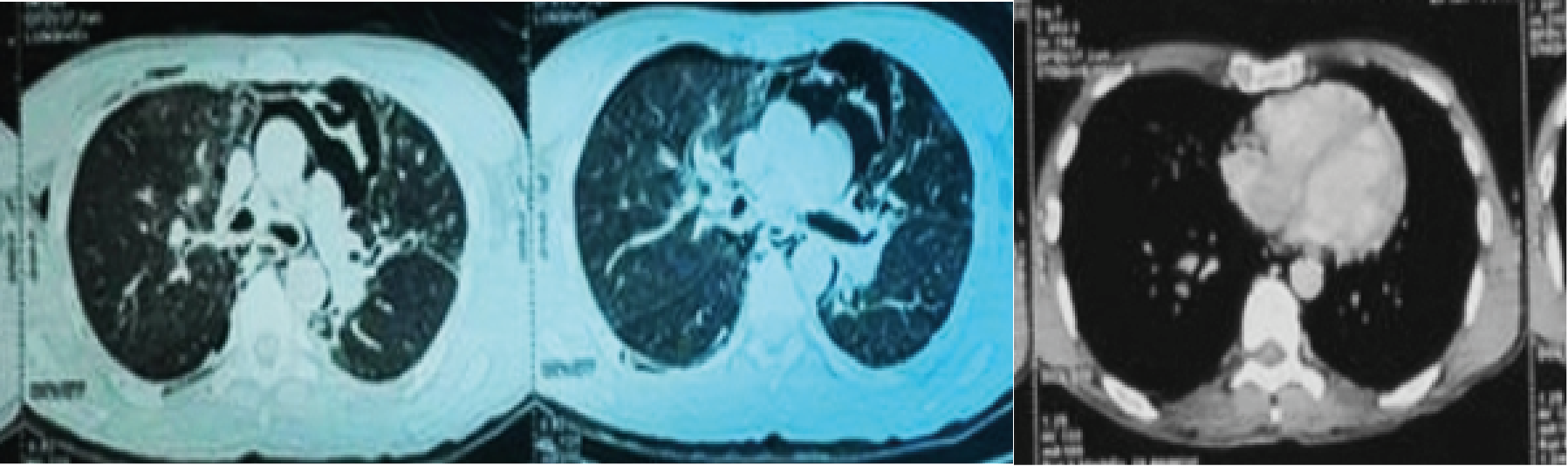
Figure 1-3: Chest CT scan.
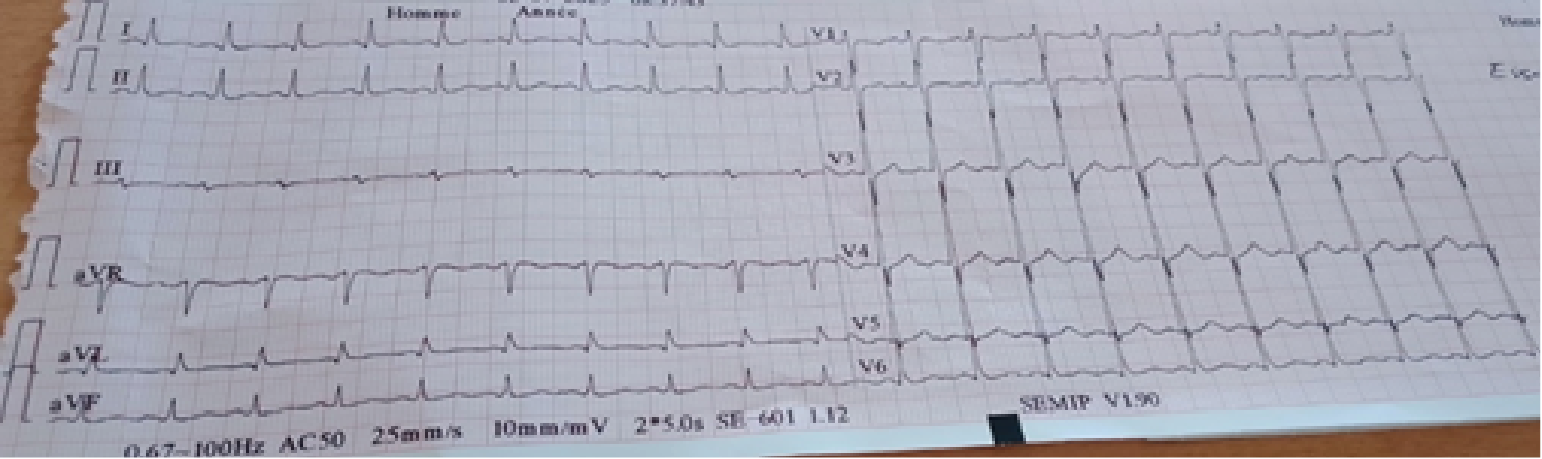
Figure 4: Electrocardiogram.
In the context of trauma, myocardial contusion is a distinct anatomo-clinical entity, often underdiagnosed due to its nonspecific clinical presentation. It results from sudden deceleration of the thorax, compressing the heart between the sternum and spine [11-14]. This can cause intramyocardial hemorrhage, rupture of intracardiac structures (valves, septum), and conduction disturbances [2].
The severity of lesions depends on the impact intensity and associated thoracic injuries [12].
Clinical presentation is variable, especially in polytrauma patients. This explains the pulmonary signs (pneumothorax) observed in our case that helped uncover cardiac involvement. Common symptoms include dyspnea, chest pain, palpitations, hypotension, and signs of cardiogenic shock [12]. Complications may include acute heart failure, arrhythmias (extrasystoles, Atrioventricular block, ventricular tachycardia), and occasionally myocardial rupture [2, 7].
Electrical abnormalities are early and transient, with ECG changes such as AV block, bundle branch block, ventricular or supraventricular arrhythmias, and ST/T wave alterations. However, troponin assays have limited sensitivity and predictive value [4, 9].
Echocardiography is useful for diagnosis by identifying segmental wall motion abnormalities, pericardial effusion, and evaluating systolic function [8]. Cardiac MRI is very helpful to assess myocardial damage and distinguish contusion from infarction [15-18]. Definitive diagnosis requires histopathological examination.
Treatment is mainly symptomatic, involving hemodynamic support with fluid resuscitation and inotropes in case of heart failure, management of arrhythmias (beta-blockers, amiodarone, cardioversion if necessary), and regular biological, electrical, and echocardiographic monitoring [10, 13].
Recent data suggests lidocaine may help restore contractility after contusion [11]. Surgical repair is indicated only in rare cases of myocardial or valvular rupture (16).
Prognosis depends on contusion severity and associated injuries. Minor forms generally evolve favorably without sequelae [17], while severe cases can lead to major complications (malignant arrhythmias, cardiogenic shock, or rarely, myocardial rupture) [18].
In cases of blunt chest trauma, myocardial contusion should always be considered, especially in the presence of dyspnea, chest pain, ECG abnormalities, or elevated troponin levels [4, 15]. There is no accessible gold standard, and the diagnosis is usually made using a combination of several diagnostic tools. Appropriate monitoring helps prevent serious complications.
- Valette S., Nouette-Gaulain K., Chardon P., Roustan JP, Ryckwaert Y., et al. (2007) [Delayed tamponade and traumatic myocardial contusion: evaluate the risk after blunt chest trauma]. Ann Fr Anesth Reanim 26: 593-595. [Crossref]
- Roland J., Seoudi HM., Albus RA., Fakhry SM (2009) Right atrial rupture from blunt thoracic trauma in a 4-year-old child. Pediatr Emerg Care 25: 188-189. [Crossref]
- Leite L., Goncalves L., Nuno VD. (2017) Lésions cardiaques dues à un traumatise: revue et études de cas. J Forensic Leg Med 52: 30-34.
- Namrata G., Parshotam LG., Abhinav S., Tej KK., Navjot B., et al. (2015) Évaluation de la contusion myocardique à l'aide de marqueurs biochimiques chez les patients traumatisés thoraciques. J Evol Med Dent Sci 4: 12015-12025.
- Clancy, K., Velopulos, C., Bilaniuk, J. W., et al. (2012) Screening for blunt cardiac injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 73: S301–S306. [Crossref]
- Robert E., de La Coussaye JE., Aya AG., Bertinchant JP., Polge A., FabbroPeray P (2000) Mechanisms of ventricular arrhythmias induced by myocardial contusion: a high-resolution mapping study in left ventricular rabbit heart. Anesthesiology 92:1132–1143. [Crossref]
- Bahar AM., Nouri M., Alizadeh L., Namvar F., Asadi M (2014) Estimated incidence of cardiac contusion using transthoracic echocardiography in patients suffering from severe blunt trauma to the chest. Acta Chir Belg 114: 105-109. [Crossref]
- Salim A., Velmahos GC., Jindal A., Chan L., Vassiliu P., et al. (2001) Clinically significant blunt cardiac trauma: role of serum troponin levels combined with electrocardiographic findings. J Trauma 50: 237-243. [Crossref]
- Contusion myocardique J. L’Hermite., J.P. Bertinchant., J.E. de La Coussaye (2001) Fédération anesthésie-douleur-urgences-réanimation, 5, rue Hoche, 30 029 Nîmes, France ; 2 service de cardiologie, centre hospitalier universitaire de Nîmes, hôpital Gaston-Doumergue, 5, rue Hoche, 30029 Nîmes cedex 09, France.
- Q Pu, J X Mazoit, L S Cao, W Mao, K Samii (1996) Effect of lignocaine in myocardial contusion: an experiment on rabbit isolated heart. Br J Pharmacol 118:1072-1078. [Crossref]
- Van Lieshout EMM, Verhofstad MHJ, Van Silfhout DJT, Dubois EA (2001) Diagnostic approach for myocardial contusion: a retrospective evaluation of patient data and review of the literature. Eur J Trauma Emerg Surg 47: 1259-1272. [Crossref]
- Thiele H, Ohman EM, Desch S, Eitel I., de Waha S (2015) Management of cardiogenic shock. Eur Heart J 36: 1223-1230. [Crossref]
- R. Jouffroy (2021) Thoracic trauma: diagnostic and therapeutic strategy. EMC Anesth Reanim.
- Berroeta C, Provencher S,. Mongredien A, Lasocki S, Benessiano., et al. (2006) The value of cardiac troponin-i as a biochemical markers of acute coronary syndromes compared with other traditional markers. Bull. Egypt. Soc. Physiol. Sci. 26.
- Prise en charge thérapeutique initiale des traumatismes thoraciques fermés et filière d’aval (2000) In SRLF, Ed actualités en réanimation et urgences. Paris : Elsevier 347-56
- Maenza R.L., Seaberg D., D’Amico F (1996) A meta-analysis of blunt cardiac trauma: ending myocardial confusion. Am J Emerg Med 14: 237-244. [Crossref]
- Lindstaedt M., Germing A., Lawo T., von Dryander S., Jaeger D., et al. (2002) Acute and long-term clinical significance of myocardial contusion following blunt thoracic trauma: results of a prospective study. J Trauma 52: 479-485. [Crossref]
- Burrell AJ., Kaye DM., Fitzgerald MC., Cooper DJ., Hare JL., et al. (2017) Cardiac magnetic resonance imaging in suspected blunt cardiac injury: A prospective, pilot, cohort study. Injury 48: 1013-1019. [Crossref]